D-Well, Cholecalciferol
- 1. Introduction to D-Well (Cholecalciferol)
- 2. Composition and Formulation
- 3. Mechanism of Action How D-Well Works
- 4. Approved Uses of D-Well (Vitamin D3)
- 5. Off-Label and Emerging Uses of Cholecalciferol
- 5.1 Immune System Support and Infection Risk Reduction
- 5.2 Adjunctive Use in Autoimmune Diseases
- 5.3 Role in Diabetes and Insulin Sensitivity
- 5.4 Cardiovascular Health and Blood Pressure Support
- 5.5 Mood Disorders and Depression Management
- 5.6 Support in Polycystic Ovary Syndrome (PCOS)
- 5.7 Vitamin D in Obesity and Metabolic Syndrome
- 5.8 Potential Role in Cancer Prevention Research
- 6. Dosage and Administration Guidelines
- 7. Administration in Special Populations
- 8. Cholecalciferol Side Effects
- 9. Drug, Food, and Supplement Interactions
- 10. Warnings and Safety Information
- 11. Contraindications
- 12. Careful Administration and Important Precautions
- 12.1 Use the Lowest Effective Dose
- 12.2 Avoid Concurrent High-Dose Vitamin D from Multiple Sources
- 12.3 Regular Laboratory Monitoring in Long-Term Therapy
- 12.4 Precautions in Patients with Cardiovascular Disease
- 12.5 Considerations in Patients with Malabsorption or Bariatric Surgery
- 12.6 Individualized Dosing Based on Risk Factors
- 13. Overdosage and Management
- 14. Storage and Stability
- 15. Handling Precautions
- 16. Patient Counseling and Practical Tips
1. Introduction to D-Well (Cholecalciferol)
1.1 What is D-Well? Overview of Vitamin D3 Supplementation
D-Well contains cholecalciferol, commonly known as Vitamin D3, an essential nutrient required for optimal skeletal integrity and metabolic balance. It is widely prescribed to prevent and correct vitamin D deficiency. This deficiency, often silent, can progressively compromise bone density and systemic health.
D-Well is used when dietary intake or sunlight exposure is insufficient. It helps restore physiological vitamin D levels and supports long-term wellness.
1.2 Therapeutic Classification: Fat-Soluble Vitamin and Hormone Precursor
Cholecalciferol belongs to the group of fat-soluble vitamins. However, its biological behavior resembles that of a prohormone. Once metabolized, it is converted into calcitriol, the hormonally active form that regulates calcium metabolism and cellular function.
1.3 Importance of Vitamin D in Human Health
Vitamin D plays a multifaceted role in maintaining systemic equilibrium:
- Enhances calcium and phosphorus absorption
- Supports bone mineralization
- Maintains muscle strength
- Modulates immune response
- Contributes to neuromuscular coordination
Deficiency has been associated with osteoporosis, fractures, muscle weakness, and impaired immunity.
1.4 Prevalence and Risk Factors for Vitamin D Deficiency
Vitamin D insufficiency is increasingly prevalent worldwide. Contributing factors include limited sun exposure, aging, darker skin pigmentation, obesity, malabsorption disorders, and chronic kidney or liver disease.
2. Composition and Formulation
2.1 Active Ingredient: Cholecalciferol (Vitamin D3)
2.2 Available Strengths and Dosage Forms
D-Well is manufactured in multiple pharmaceutical forms to accommodate varying clinical needs:
- Tablets and capsules
- Softgel formulations
- Oral drops for pediatric use
- Sachets or high-dose preparations
2.3 Excipients and Inactive Ingredients
Formulations may include stabilizers, carriers, and lipid-based vehicles that enhance solubility and absorption. These components vary by manufacturer and dosage form.
2.4 Differences Between Cholecalciferol (D3) and Ergocalciferol (D2)
Vitamin D3 demonstrates superior potency and longer duration of action compared to vitamin D2 (ergocalciferol). It produces more sustained increases in serum vitamin D levels.
2.5 Bioavailability and Absorption Characteristics
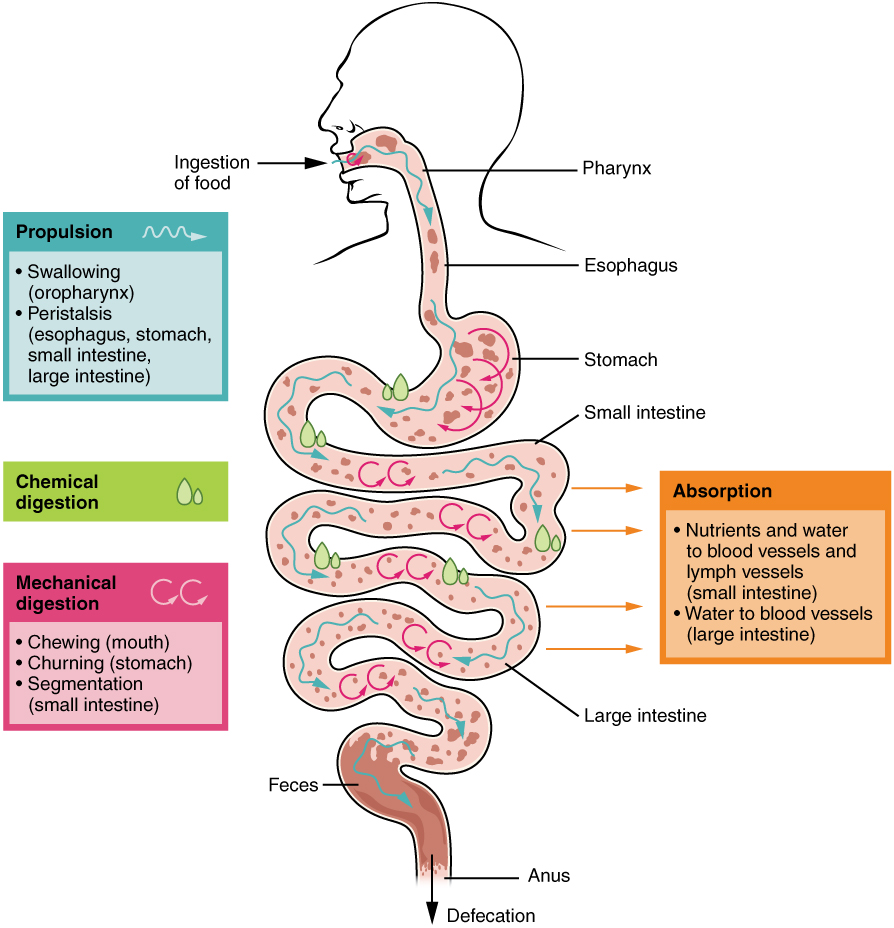
Being fat-soluble, cholecalciferol is optimally absorbed when taken with meals containing dietary fat. Lipid-based formulations further enhance bioavailability.
Cholecalciferol vs ergocalciferol
Ergocalciferol (D2) comes from plants/fungi and is less potent/stable than cholecalciferol (D3), which comes from animals/sunlight and is more effective at raising vitamin D levels.
Calcitriol vs cholecalciferol
Cholecalciferol is an inactive precursor synthesized in the skin or taken as a supplement that requires conversion by the liver and kidneys to become active. Calcitriol is the final, biologically active hormone form that is absorbed by the body.
3. Mechanism of Action How D-Well Works
3.1 Conversion of Cholecalciferol to Active Vitamin D (Calcitriol)
After ingestion, cholecalciferol undergoes hydroxylation in the liver and kidneys to form calcitriol. This metabolite acts as a hormone influencing calcium balance and gene expression.
3.2 Role in Calcium and Phosphorus Homeostasis
Calcitriol increases intestinal absorption of calcium and phosphorus. It also reduces renal excretion and supports skeletal mineralization.
3.3 Effects on Bone Mineralization and Skeletal Health

3.4 Impact on Parathyroid Hormone Regulation
3.5 Extra-Skeletal Actions
Emerging evidence suggests broader physiological effects:
- Immune modulation
- Muscle function enhancement
- Cellular growth regulation
- Anti-inflammatory activity
4. Approved Uses of D-Well (Vitamin D3)
4.1 Prevention and Treatment of Vitamin D Deficiency
D-Well is primarily indicated for individuals with documented or suspected vitamin D deficiency.
4.2 Management of Osteoporosis
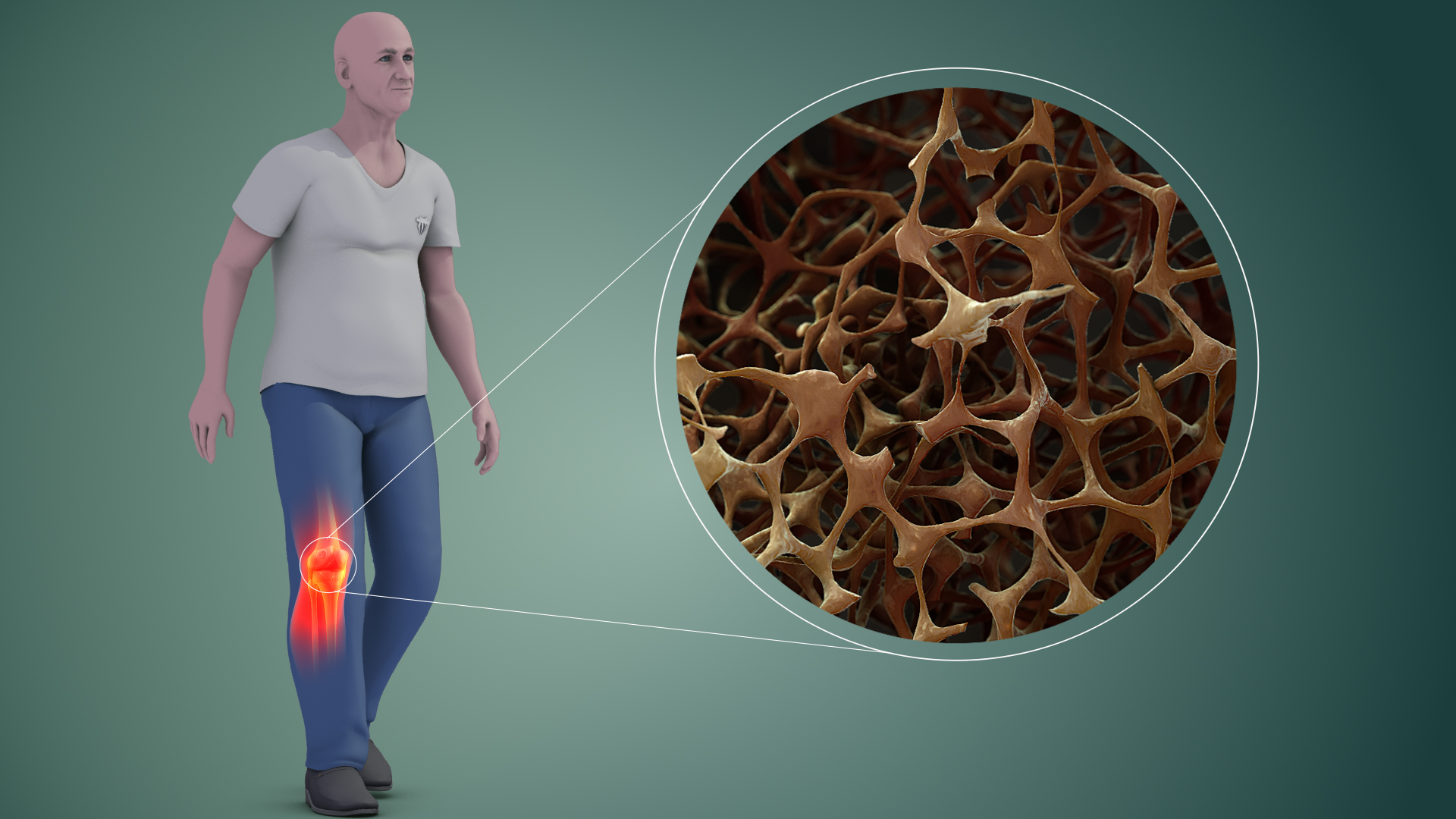
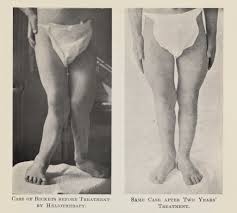
4.3 Treatment of Osteomalacia and Rickets
D-Well supports bone mineralization in conditions characterized by defective bone formation.
4.4 Support in Hypocalcemia and Hypophosphatemia
By enhancing mineral absorption, it helps correct low calcium and phosphorus levels.
4.5 Adjunct Therapy in Chronic Kidney Disease Related Bone Disorders
Patients with renal impairment may require vitamin D supplementation to maintain mineral balance.
4.6 Prevention of Secondary Hyperparathyroidism
Supplementation helps regulate parathyroid hormone levels in at-risk populations.
5. Off-Label and Emerging Uses of Cholecalciferol
5.1 Immune System Support and Infection Risk Reduction
5.2 Adjunctive Use in Autoimmune Diseases
Supplementation is being explored in conditions such as multiple sclerosis and rheumatoid arthritis.
5.3 Role in Diabetes and Insulin Sensitivity
Vitamin D may influence glucose metabolism and insulin responsiveness.
5.4 Cardiovascular Health and Blood Pressure Support
Observational studies suggest a link between adequate vitamin D levels and cardiovascular health.
5.5 Mood Disorders and Depression Management
Low vitamin D levels have been associated with mood disturbances and seasonal affective symptoms.
5.6 Support in Polycystic Ovary Syndrome (PCOS)
Supplementation may improve metabolic and hormonal parameters in PCOS.
5.7 Vitamin D in Obesity and Metabolic Syndrome
Higher body fat may reduce vitamin D bioavailability, necessitating supplementation.
5.8 Potential Role in Cancer Prevention Research
Research is ongoing regarding its influence on cellular differentiation and tumor regulation.
6. Dosage and Administration Guidelines
6.1 Recommended Daily Allowance by Age Group
Daily requirements vary according to age, physiological status, and risk factors.
6.2 Therapeutic Dosing for Vitamin D Deficiency
Higher doses may be prescribed for short-term correction under medical supervision.
6.3 Maintenance Dosing Strategies
Maintenance therapy helps sustain optimal serum vitamin D levels.
6.4 High-Dose (Loading) Regimens
Loading doses may be used in severe deficiency cases.
6.5 Administration Instructions
Take D-Well with meals, preferably those containing fat, to enhance absorption.
6.6 Duration of Therapy and Monitoring
Periodic laboratory monitoring may be recommended during long-term use.

6.7 Missed Dose and Dose Adjustment
If a dose is missed, it should be taken as soon as remembered unless close to the next scheduled dose.
7. Administration in Special Populations
7.1 Administration to Elderly Patients
Supplementation supports bone density, muscle strength, and fall prevention.

7.2 Use in Pregnant Women
Adequate vitamin D is important for maternal and fetal bone development. Dosing should follow medical guidance.
7.3 Administration to Nursing Mothers
Maternal supplementation helps maintain adequate vitamin D levels in breastfed infants.
7.4 Pediatric Use
Infants and children may require supplementation to prevent rickets and support growth.

7.5 Use in Malabsorption Syndromes
Higher or specialized dosing may be required in gastrointestinal disorders.
7.6 Renal or Hepatic Impairment
Patients with organ dysfunction require careful monitoring and individualized dosing.
8. Cholecalciferol Side Effects
8.1 Overview of Safety Profile
D-Well is generally well tolerated when used within recommended doses.
8.2 Common Side Effects
- Mild gastrointestinal discomfort
- Nausea or vomiting
- Constipation
- Fatigue or generalized weakness

8.3 Signs of Excess Vitamin D (Hypervitaminosis D)
Excessive intake may lead to toxic accumulation.
8.4 Symptoms of Hypercalcemia
- Loss of appetite
- Frequent urination
- Kidney stones
- Confusion or cardiac irregularities
8.5 When to Seek Medical Attention
Medical evaluation is necessary if symptoms of toxicity or persistent adverse effects occur.
9. Drug, Food, and Supplement Interactions
9.1 Interaction with Calcium Supplements and Multivitamins
Concurrent use may increase the risk of excessive calcium levels.
9.2 Effects of Corticosteroids
Long-term corticosteroid therapy may reduce vitamin D metabolism.
9.3 Interaction with Anticonvulsants
Medications such as phenytoin and phenobarbital can accelerate vitamin D breakdown.
9.4 Cholestyramine and Fat-Absorption Interference
Fat-binding agents may impair vitamin D absorption.
9.5 Thiazide Diuretics
Combined use may increase the risk of hypercalcemia.
9.6 Interaction with Orlistat
Weight-loss medications that reduce fat absorption may lower vitamin D availability.

9.7 Food Factors Affecting Absorption
Vitamin D absorption improves when taken with meals containing healthy fats.
10. Warnings and Safety Information
10.1 Risk of Vitamin D Toxicity with Excessive Intake
Although cholecalciferol is essential for health, excessive intake may lead to serious complications. Vitamin D toxicity typically results from prolonged high-dose supplementation rather than dietary sources or sunlight exposure.
Excessive levels increase intestinal calcium absorption, which may lead to:
- Hypercalcemia
- Nausea and vomiting
- Loss of appetite
- Muscle weakness
- Confusion or lethargy
Adherence to recommended dosing is critical. More is not better; physiological balance is the therapeutic objective.
10.2 Monitoring Serum Calcium and Vitamin D Levels
Patients receiving long-term or high-dose therapy should undergo periodic laboratory evaluation. Monitoring typically includes:
- Serum 25-hydroxyvitamin D levels
- Serum calcium
- Renal function tests
- Urinary calcium when indicated
Regular assessment helps prevent cumulative toxicity and ensures therapeutic adequacy.
10.3 Caution in Patients with Kidney Stones
Individuals with a history of nephrolithiasis require careful supervision. Increased calcium absorption may elevate urinary calcium excretion, potentially promoting stone formation.
Moderate dosing and adequate hydration are essential in this population.

10.4 Risk in Patients with Granulomatous Diseases (e.g., Sarcoidosis)
Granulomatous disorders may enhance the extrarenal conversion of vitamin D to its active form. This dysregulated activation increases the risk of hypercalcemia even at standard doses.
Conditions requiring caution include:
- Sarcoidosis
- Tuberculosis
- Certain lymphomas
10.5 Long-Term High-Dose Safety Considerations
Chronic administration of supraphysiological doses may lead to insidious complications. Potential risks include vascular calcification, renal impairment, and soft tissue mineralization. Long-term therapy should be individualized and medically supervised.
11. Contraindications
11.1 Known Hypersensitivity to Cholecalciferol or Formulation Components
D-Well should not be used in individuals with a documented hypersensitivity to cholecalciferol or any excipients contained in the formulation.
11.2 Hypercalcemia or Hypercalciuria
Supplementation is contraindicated in patients with elevated serum or urinary calcium levels, as additional vitamin D may exacerbate metabolic imbalance.
11.3 Vitamin D Toxicity (Hypervitaminosis D)
Patients with pre-existing vitamin D excess should avoid further supplementation until levels normalize.
11.4 Severe Renal Impairment with Altered Calcium Metabolism
Advanced renal disease may impair vitamin D metabolism and calcium regulation. In such cases, specialized vitamin D analogs and careful monitoring may be required.
11.5 Conditions Associated with Increased Calcium Sensitivity
Use is contraindicated or requires strict medical supervision in disorders characterized by heightened calcium sensitivity, such as primary hyperparathyroidism.
12. Careful Administration and Important Precautions
12.1 Use the Lowest Effective Dose
Therapy should aim to restore and maintain adequate vitamin D levels without exceeding physiological requirements. Dose escalation should be guided by laboratory results.
12.2 Avoid Concurrent High-Dose Vitamin D from Multiple Sources
Patients should be advised to review all supplements and fortified products. Hidden sources of vitamin D may include:
- Multivitamins
- Calcium combinations
- Fortified foods
- Over-the-counter supplements
12.3 Regular Laboratory Monitoring in Long-Term Therapy
Periodic testing ensures therapeutic efficacy while minimizing the risk of cumulative toxicity.
12.4 Precautions in Patients with Cardiovascular Disease
Excess calcium levels may contribute to vascular calcification. Patients with cardiovascular conditions should receive conservative dosing and clinical monitoring.
12.5 Considerations in Patients with Malabsorption or Bariatric Surgery
12.6 Individualized Dosing Based on Risk Factors
Age, body weight, comorbid conditions, and baseline vitamin D status should guide dosing decisions. Personalized therapy improves safety and effectiveness.
13. Overdosage and Management
13.1 Causes of Vitamin D Overdose
Overdose most commonly results from excessive supplementation, dosing errors, or prolonged intake of high-potency preparations without medical supervision.
13.2 Clinical Features of Hypervitaminosis D
Symptoms are primarily related to hypercalcemia and may include:
- Persistent nausea and vomiting
- Polyuria and dehydration
- Weakness and fatigue
- Confusion or altered mental status
13.3 Complications: Kidney Damage and Soft Tissue Calcification
Severe toxicity may result in nephrocalcinosis, renal insufficiency, and calcification of vascular or soft tissues. These complications may be irreversible if not promptly addressed.
13.4 Emergency Management and Treatment Strategies
Management includes immediate discontinuation of vitamin D and calcium sources. Medical treatment may involve:
- Intravenous hydration
- Loop diuretics
- Corticosteroids or bisphosphonates in severe cases
- Close monitoring of electrolytes and renal function
13.5 Prevention of Accidental Overdose
Clear labeling, adherence to prescribed doses, and patient education are essential preventive measures.
14. Storage and Stability
14.1 Recommended Storage Conditions
D-Well should be stored at controlled room temperature, protected from excessive heat, moisture, and direct sunlight. Environmental stability preserves potency.
14.2 Shelf Life and Expiry Considerations
Products should not be used beyond the expiration date. Degradation over time may reduce therapeutic effectiveness.
14.3 Storage of Liquid or Drop Formulations
Liquid preparations should be tightly closed after use and stored according to manufacturer recommendations to prevent contamination and oxidation.
14.4 Safe Storage Away from Children
Vitamin D products should be kept out of reach of children to prevent accidental ingestion and toxicity.
15. Handling Precautions
15.1 Proper Handling and Dispensing Practices
Dispense the product using clean hands and avoid exposure to humidity or contaminants. Packaging integrity should be maintained.
15.2 Avoid Contamination of Liquid Preparations
Droppers should not come into contact with surfaces, skin, or oral structures to prevent microbial contamination.
15.3 Accurate Measurement for Pediatric Dosing
Precise dosing is critical in infants and children. Use calibrated measuring devices rather than household utensils.
15.4 Patient Education for Safe Home Use
Patients should be instructed on correct dosing, storage, and the importance of avoiding unsupervised dose adjustments.
16. Patient Counseling and Practical Tips
16.1 Importance of Adherence to Prescribed Dose
Consistent dosing ensures therapeutic stability. Irregular intake may compromise treatment outcomes or increase the risk of imbalance.
16.2 Dietary Sources of Vitamin D and Sunlight Exposure
Supplementation should be complemented by natural sources when appropriate:
- Fatty fish such as salmon and mackerel
- Fortified dairy and cereals
- Moderate sunlight exposure
16.3 Signs of Deficiency vs. Excess
Patients should be aware of clinical indicators:
- Deficiency: bone pain, muscle weakness, fatigue
- Excess: nausea, frequent urination, confusion
16.4 When to Schedule Follow-Up Testing
Follow-up laboratory testing is typically recommended after initiation of therapy, dose adjustments, or prolonged supplementation.
16.5 Lifestyle Measures to Support Bone and Overall Health
Optimal outcomes are achieved through a comprehensive approach:
- Balanced calcium intake
- Regular weight-bearing exercise
- Adequate protein consumption
- Avoidance of smoking and excessive alcohol
Such measures enhance skeletal resilience and contribute to long-term metabolic health.
D-Well, Cholecalciferol FAQ
- What is vitamin D cholecalciferol good for?
- Can I take cholecalciferol every day?
- Is colecalciferol the same as vitamin D?
- Does cholecalciferol have side effects?
- What to avoid when taking cholecalciferol?
- What foods are high in cholecalciferol?
- How does vitamin D affect sleep?
- What are the side effects of too much cholecalciferol?
- Can colecalciferol affect sleep?
- What are symptoms of low cholecalciferol?
- Can cholecalciferol cause weight gain?
- Can cholecalciferol cause kidney stones?
- Does cholecalciferol increase cholesterol?
- Is cholecalciferol bad for the liver?
- What organ produces cholecalciferol?
- Does colecalciferol make you sleepy?
- Does cholecalciferol cause high calcium?
- Who should not take cholecalciferol?
- When to take cholecalciferol, morning or night?
- Which food has cholecalciferol?
What is vitamin D cholecalciferol good for?
It is used to treat vitamin D deficiency.
Can I take cholecalciferol every day?
Yes
Is colecalciferol the same as vitamin D?
Colecalciferol is a form of vitamin D
Does cholecalciferol have side effects?
- Hypercalcemia
- Weakened bones
- Kidney and heart damage
What to avoid when taking cholecalciferol?
- Laxatives
What foods are high in cholecalciferol?
- Fatty fish
- Beef liver
- Egg yolk
- Cheese
How does vitamin D affect sleep?
Vitamin deficiency can lead to sleep difficulties
What are the side effects of too much cholecalciferol?
- Stomachache
- Vomiting
- Frequent urination
Can colecalciferol affect sleep?
Yes
What are symptoms of low cholecalciferol?
- Fatigue
- Tiredness
- Bone pain
- Hair loss
- Appetite loss
- Depression
Can cholecalciferol cause weight gain?
No
Can cholecalciferol cause kidney stones?
Yes
Does cholecalciferol increase cholesterol?
No
Is cholecalciferol bad for the liver?
Yes
What organ produces cholecalciferol?
Kidneys
Does colecalciferol make you sleepy?
Yes
Does cholecalciferol cause high calcium?
Yes
Who should not take cholecalciferol?
- Patient with kidney problems
When to take cholecalciferol, morning or night?
Morning
Which food has cholecalciferol?
- Fatty fish
- Egg yolks
Popular Products





Similar Product