1. Introduction to Misoprost / Misoprostol
1.1 Overview of Misoprostol as a Prostaglandin E1 Analog
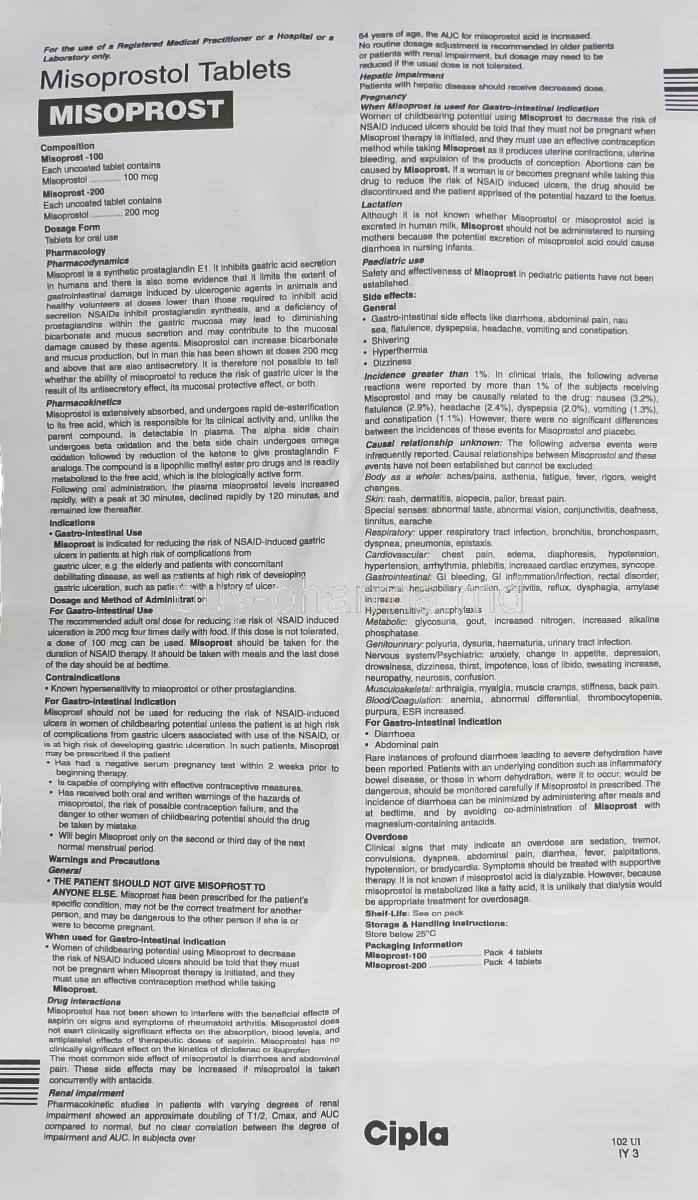
Misoprostol is a synthetic analog of prostaglandin E1 (PGE1). It mimics the activity of naturally occurring prostaglandins in the body, particularly within the gastrointestinal tract and the uterus. By binding to specific prostaglandin receptors, misoprostol exerts cytoprotective effects on the gastric mucosa and stimulates uterine contractions.
This dual profile explains why the same molecule is used both as a gastroprotective agent and as an obstetric and gynecologic tool under strict medical supervision.
1.2 Historical Background and Medical Adoption
Initially developed and approved for the prevention of nonsteroidal anti-inflammatory drug (NSAID)–induced gastric and duodenal ulcers, misoprostol was rapidly recognized for its potent uterotonic properties. Over time, it became integrated into various obstetric protocols, including induction of labor and management of postpartum hemorrhage, particularly in resource-limited settings.
- Gastroenterology: introduced as a mucosal Protectant.
- Obstetrics and gynecology: later adopted for carefully controlled uterine indications.
- Public health: incorporated into global maternal health strategies, following evidence-based guidelines.
1.3 Brand Names, Generics, and Global Availability
Misoprostol is marketed under various brand names and generic labels worldwide. It may appear as a stand-alone product or in fixed-dose combinations with other agents (for example, with certain NSAIDs for ulcer prophylaxis).
Availability, brand naming conventions, and approved indications can differ substantially between countries, reflecting local regulatory decisions and public health priorities.
1.4 Regulatory Status in Different Countries
Regulatory authorities, such as the U.S. Food and Drug Administration (FDA), European Medicines Agency (EMA), and national agencies in Asia, Latin America, and Africa, define how misoprostol may be marketed and used. In some regions, it is approved primarily for ulcer prevention and specific obstetric indications, while other uses remain off-label.
Legal status, prescription requirements, and allowable indications must always be checked within the country of use, as these frameworks also govern who may prescribe and administer misoprostol and under what conditions.
2. Composition and Formulations
2.1 Active Ingredient: Misoprostol
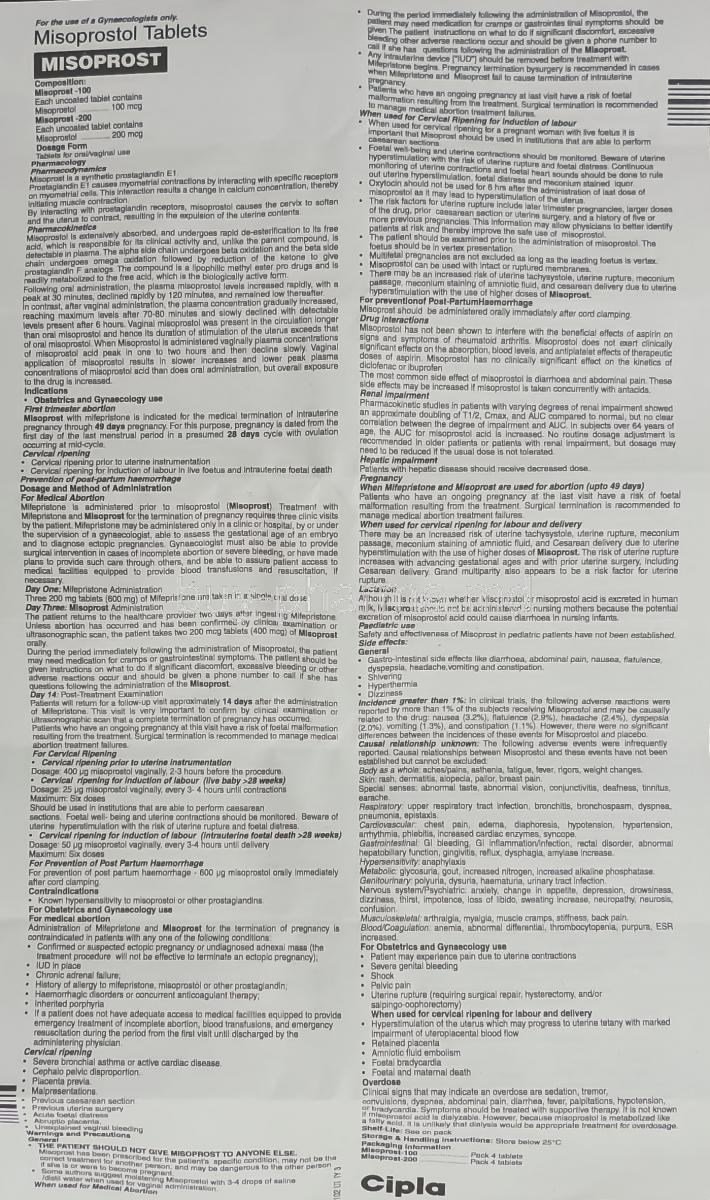
The active ingredient in Misoprost-type products is misoprostol, a prostaglandin E1 analog. It is usually formulated as a tablet containing a precisely measured microgram dose to allow predictable pharmacological effects and dosing flexibility.
2.2 Available Dosage Forms (Tablets, Buccal, Sublingual, Vaginal)
Misoprostol is commonly supplied as:
- Oral tablets for gastroprotection and some obstetric applications.
- Tablets used via buccal route (placed in the cheek) for certain protocols.
- Sublingual administration (under the tongue) for rapid absorption.
- Vaginal administration for localized effects in the cervix and uterus.
Although the tablet itself is often identical, the route of administration profoundly influences absorption, peak concentrations, and clinical effect.
2.3 Inactive Ingredients and Stability Considerations
Beyond the active compound, misoprostol tablets contain excipients such as fillers, binders, and stabilizers. These help maintain tablet integrity, enhance shelf life, and ensure consistent disintegration.
Misoprostol is relatively sensitive to moisture and heat. The formulation therefore aims to minimize degradation and maintain potency throughout the stated shelf life.
2.4 Pharmaceutical Strengths and Packaging
Standard strengths may vary by manufacturer, commonly expressed in micrograms. Blister packaging is frequently used to protect tablets from humidity and to help patients track doses.
- Unit-dose blister packs to protect each tablet.
- Clearly labeled strength to avoid dosing errors.
- Package inserts containing detailed prescribing information for healthcare professionals.
3. Mechanism of Action (How Misoprostol Works)
3.1 Prostaglandin Receptor Activation and Physiologic Effects
Misoprostol binds to specific prostaglandin E (EP) receptors located in various tissues. Activation of these receptors results in several key effects:
- Increased mucus and bicarbonate secretion in the stomach.
- Reduced gastric acid secretion.
- Enhanced uterine smooth muscle contractility.
- Cervical softening and dilation.
This receptor-level interaction underlies both its protective gastrointestinal action and its uterotonic activities.
3.2 Gastric Mucosal Protection Mechanism
Within the gastrointestinal tract, misoprostol:
- Stimulates mucous cell secretion, forming a protective barrier against acid.
- Enhances bicarbonate secretion, helping to neutralize gastric acid.
- Improves mucosal blood flow, supporting tissue repair and resilience.
Collectively, these actions reduce the risk of NSAID-induced mucosal injury and ulcer formation when used as directed.
3.3 Uterotonic Activity and Cervical Ripening
Misoprostol increases the frequency and intensity of uterine contractions by acting directly on uterine smooth muscle. In the cervix, it promotes softening (ripening) and dilation, facilitating labor or gynecologic procedures.
The uterotonic effect is powerful and must be carefully titrated under expert supervision to avoid excessive stimulation, which could jeopardize maternal or fetal safety.
3.4 Time to Onset and Duration of Action
The onset of action varies with route of administration:
- Oral and sublingual: relatively rapid absorption and onset.
- Buccal: slightly slower but sustained absorption.
- Vaginal: slower onset with more prolonged uterine effect in many protocols.
Duration of action is typically a few hours, but clinical effects, such as cervical ripening or bleeding patterns, may persist beyond the pharmacokinetic window.
3.5 Differences Between Oral, Sublingual, Buccal, and Vaginal Routes
Each route has specific advantages and limitations:
- Oral: convenient but subject to first-pass metabolism and gastrointestinal side effects.
- Sublingual: rapid peak plasma levels; useful when a brisk effect is needed.
- Buccal: controlled absorption; may reduce some gastrointestinal adverse effects.
- Vaginal: localized effect on the uterus and cervix; often used for induction of labor or certain gynecologic indications.
Choice of route is individualized and guided by evidence-based protocols and clinical judgment.
4. Approved Medical Uses
4.1 Prevention of Gastric and Duodenal Ulcers
4.1.1 NSAID-Induced Ulcer Prevention
Misoprostol is approved in many regions to prevent gastric and duodenal ulcers associated with chronic NSAID therapy. Patients requiring long-term NSAID treatment, particularly those at higher risk for gastrointestinal complications, may be prescribed misoprostol to mitigate mucosal injury.
4.1.2 Role in Chronic NSAID Therapy
For individuals who cannot discontinue NSAIDs, misoprostol can be a key component of gastroprotective strategy, alongside lifestyle modifications and other acid-suppressive therapies where appropriate. The objective is to maintain anti-inflammatory benefits while reducing ulcer risk.
4.2 Induction of Labor (Where Approved)
4.2.1 Cervical Ripening Protocols
In some countries and settings, misoprostol is authorized for induction of labor at or near term under hospital-level monitoring. It assists with cervical ripening, making the cervix softer, thinner, and more dilated, which facilitates the onset of labor and progression of childbirth.
4.2.2 Uterine Contraction Stimulation
Once administered, misoprostol enhances uterine contractility. Clinical teams carefully select dose, route, and dosing intervals based on maternal and fetal status. Continuous or frequent monitoring of uterine activity and fetal heart rate is essential for safety.
4.3 Postpartum Hemorrhage (PPH) Management
4.3.1 Emergency Uterotonic Intervention
Postpartum hemorrhage is a leading cause of maternal morbidity and mortality worldwide. Misoprostol is included in several guidelines as an option for the prevention and management of PPH, especially in environments where injectable uterotonics or cold storage may not be readily available.
4.3.2 Comparisons With Oxytocin
Oxytocin remains the first-line uterotonic in many protocols; however, misoprostol’s stability at room temperature, oral/vaginal routes, and ease of storage make it particularly valuable in low-resource settings. Comparative effectiveness, side-effect profiles, and feasibility are all considered when selecting an agent.
5. Off-Label Uses
5.1 Medical Termination of Pregnancy (Early and Late Protocols)
Misoprostol is widely used, often in combination with other agents and under strict legal and clinical frameworks, for medical termination of pregnancy. Protocols vary by gestational age, local regulations, and clinical guidelines, and must only be followed under the direct supervision of qualified healthcare professionals.
5.2 Management of Incomplete or Missed Miscarriage
In cases of incomplete or missed miscarriage, misoprostol may be employed to promote expulsion of retained tissue, reducing the need for surgical intervention in selected patients. Clinical assessment, ultrasound evaluation, and follow-up are critical to ensure complete evacuation and to identify complications early.
5.3 Cervical Preparation Prior to Surgical Procedures (D&C, IUD Insertion)
Misoprostol can be used off-label to soften and dilate the cervix prior to procedures such as dilatation and curettage (D&C), hysteroscopy, or intrauterine device (IUD) insertion. Proper timing relative to the planned procedure optimizes cervical readiness and may reduce procedural difficulty.
5.4 Treatment of Postpartum Hemorrhage Where Oxytocin Is Not Available
In settings where first-line uterotonics are unavailable or impractical, misoprostol may serve as an alternative for treating postpartum hemorrhage. Its heat stability and ease of administration make it particularly valuable in community and low-resource environments, provided that appropriate training and follow-up are in place.
5.5 Induction of Labor (Where Off-Label)
In some countries, use of misoprostol for induction of labor remains off-label. In such contexts, its administration is guided by professional society recommendations and local standards of care, always with careful monitoring due to the risk of excessive uterine stimulation.
5.6 Combination Use With Mifepristone (Medical Abortion Regimens)
Combination regimens involving mifepristone followed by misoprostol are employed in many healthcare systems for medical abortion, consistent with local law and clinical guidelines. These regimens are highly protocolized and should only be prescribed and supervised by trained healthcare professionals who can provide counseling, follow-up, and emergency care.
5.7 Softening of Cervix for Gynecological Procedures
Beyond pregnancy-related indications, misoprostol may be used to facilitate other gynecologic interventions requiring cervical dilation, such as certain diagnostic or operative procedures. Again, individualized decision-making and formal protocols are key.
5.8 Fetal Demise Management
In cases of intrauterine fetal demise, misoprostol can be part of the management strategy to induce labor and complete delivery. Such situations are medically and emotionally complex, necessitating multidisciplinary support, clear communication, and careful dosing and monitoring.
6. Dosage and Administration
6.1 General Adult Dosing Guidelines
Dosing of misoprostol depends entirely on the indication, route of administration, and patient-specific factors. Healthcare professionals follow evidence-based guidelines, which specify dose ranges, timing, and maximum cumulative amounts to balance efficacy and safety.
Self-adjusting the dose or using misoprostol without medical supervision is unsafe and strongly discouraged.
6.2 Dosing for NSAID-Induced Ulcer Prevention
For prevention of NSAID-induced ulcers, misoprostol is typically given orally, in multiple daily doses with food. The exact regimen is chosen to achieve adequate mucosal protection while minimizing gastrointestinal side effects such as diarrhea and cramping.
6.3 Dosing for Labor Induction (Oral/Vaginal/Buccal)
When used for labor induction, carefully controlled low doses are employed, given at specified intervals and routes (oral, vaginal, or buccal) according to institutional protocols. The dosing strategy aims to achieve effective contractions without causing uterine hyperstimulation or fetal compromise.
6.4 Dosing for Medical Abortion (Monotherapy and Combined)
For medical abortion, dosing regimens are standardized in clinical guidelines and often differ by gestational age and whether misoprostol is used alone or in combination with another agent. Because of the complexity and risk, it is essential that dosing be determined and supervised by clinicians experienced in this field.
6.5 Dosing for Miscarriage Management
In the management of early pregnancy loss, clinicians select dose, route, and timing based on the type of miscarriage, gestational age, and patient preference, with close follow-up to confirm completion and detect complications such as heavy bleeding or infection.
6.6 Dosing for Postpartum Hemorrhage
In postpartum hemorrhage protocols, misoprostol is administered in specific doses and routes designed to rapidly stimulate uterine contraction. Emergency frameworks and resuscitation resources must be available, given the potential severity of PPH.
6.7 Special Instructions for Buccal, Sublingual, and Vaginal Use
When used buccally or sublingually, tablets are placed in the cheek or under the tongue and allowed to dissolve, avoiding chewing or swallowing immediately to enhance mucosal absorption. For vaginal use, tablets are placed high in the vagina, often by a clinician or under clear instruction.
Hygiene, positioning, and timing relative to procedures or examinations are all important practical considerations that are explained by healthcare professionals before use.
6.8 Missed Dose Instructions for Gastric Protection
If a dose for ulcer prevention is missed, patients are usually advised to take it when remembered unless it is nearly time for the next dose. Doubling doses is typically not recommended. Exact instructions should follow the prescribing information and the advice of the treating clinician.
7. Important Precautions
7.1 Monitoring Requirements
Misoprostol use, particularly for obstetric and gynecologic indications, necessitates careful monitoring. Depending on the indication, monitoring may include:
- Vital signs, including blood pressure and pulse.
- Uterine contraction pattern and frequency.
- Fetal heart rate surveillance during pregnancy.
- Assessment of bleeding, pain, and overall clinical status.
7.2 Risks of Uterine Rupture (High-Risk Groups)
Women with prior uterine surgery, such as cesarean section or myomectomy, may be at increased risk of uterine rupture, especially with higher doses or inappropriate regimens. These patients require individualized assessment and very cautious use, if misoprostol is considered at all.
7.3 Severe Diarrhea and Dehydration Risk
Gastrointestinal side effects can be pronounced. Severe, persistent diarrhea can lead to dehydration, electrolyte imbalance, and weakness. Patients should be instructed to maintain adequate fluid intake and to seek medical attention if symptoms become intense or prolonged.
7.4 Management of Heavy Bleeding
Misoprostol can be associated with significant vaginal bleeding in certain indications. Healthcare professionals provide clear instructions on what level of bleeding is expected and when it becomes excessive. Heavy bleeding, dizziness, faintness, or signs of shock warrant urgent evaluation.
7.5 Recognizing Signs of Incomplete Abortion
After medical abortion or miscarriage management, signs of incomplete expulsion—such as ongoing heavy bleeding, persistent pain, or fever—must be recognized early. Follow-up visits, ultrasound assessments, or laboratory tests may be used to confirm completion and identify complications.
7.6 Avoiding Use Without Medical Guidance
Because misoprostol is a potent pharmacologic agent with the potential for serious adverse outcomes, unsupervised use is unsafe. Consultation with a qualified healthcare professional is essential before starting, adjusting, or discontinuing therapy.
8. Warnings
8.1 FDA Boxed Warning and Pregnancy Risk
In some jurisdictions, misoprostol carries a boxed warning highlighting the risk of pregnancy loss, uterine rupture, and serious maternal morbidity when used improperly. It may cause birth defects or pregnancy termination if administered during pregnancy for non-obstetric indications.
8.2 Contraindications in Pregnancy (For Ulcer Treatment)
When prescribed for ulcer prevention, misoprostol is contraindicated in women who are pregnant or who may become pregnant, unless appropriate precautions are in place. Effective contraception and thorough counseling are crucial for individuals of childbearing potential receiving misoprostol for gastrointestinal indications.
8.3 Serious Gastrointestinal Reactions
Although misoprostol protects the gastric mucosa, it can also trigger significant gastrointestinal disturbances. Severe abdominal pain, persistent vomiting, or bloody stools should prompt immediate medical assessment.
8.4 Severe Uterine Hyperstimulation
Excessive uterine contractions may jeopardize fetal oxygenation and maternal safety. Hyperstimulation, with or without fetal heart rate abnormalities, requires prompt intervention – often including discontinuation of further doses and additional medical measures.
8.5 Systemic Infection and Sepsis Risk
Any procedure or process involving the uterus carries some risk of infection. Fever, foul-smelling discharge, increasing abdominal pain, or a general feeling of being acutely unwell after misoprostol use may signal infection or sepsis and must be evaluated urgently.
9. Contraindications
9.1 Known Allergy to Misoprostol or Prostaglandins
Misoprostol must not be used in individuals with hypersensitivity to misoprostol, other prostaglandins, or any component of the formulation. A history of severe allergic reaction is a clear contraindication.
9.2 Pregnant Women Using Misoprostol for Ulcer Prevention
For gastrointestinal indications, misoprostol is contraindicated in pregnant women due to the risk of uterine contractions, pregnancy loss, and fetal harm. Alternative treatments should be considered in this population.
9.3 Patients With Suspected Ectopic Pregnancy
Misoprostol is not an appropriate treatment for ectopic pregnancy. If an ectopic pregnancy is suspected, immediate specialist assessment is necessary, as delayed treatment can lead to life-threatening complications.
9.4 Uterine Scar or Previous Cesarean (Certain Doses)
In women with previous cesarean sections or other uterine scars, some misoprostol regimens may be contraindicated because of elevated risk of uterine rupture. Any use in this population must be carefully weighed and follow strict protocols where permitted.
9.5 Cardiovascular Instability
Patients with unstable cardiovascular status may be at higher risk of complications related to bleeding, fluid shifts, or systemic reactions. In such individuals, misoprostol use requires careful assessment and monitoring, and may be inappropriate in some scenarios.
9.6 Inflammatory Bowel Disease (Severe Diarrhea Risk)
In patients with inflammatory bowel disease or other conditions predisposing to severe diarrhea, misoprostol can exacerbate symptoms and should be used with great caution or avoided, depending on clinical judgment.
10. Side Effects
10.1 Overview of Possible Adverse Effects
Misoprostol can cause a spectrum of side effects, ranging from mild and transient to serious and potentially life-threatening. Many adverse effects are dose-related and become more likely with higher cumulative doses or when used outside established protocols.
10.2 Gastrointestinal Side Effects
10.2.1 Diarrhea
Diarrhea is among the most common adverse effects. It may be mild and self-limited, but in some cases it can be profuse, leading to dehydration and electrolyte imbalance. Adequate fluid intake and medical review are important if symptoms are severe.
10.2.2 Abdominal Cramping
Cramping may arise from both gastrointestinal smooth muscle activity and uterine contractions. While mild cramping is often expected, intense or persistent pain requires clinical evaluation to exclude complications.
10.2.3 Nausea and Vomiting
Nausea and occasional vomiting can occur, particularly with oral administration. Dividing doses, taking medication with food for gastric indications, and using supportive antiemetic therapy may help, as advised by a clinician.
10.3 Gynecologic and Obstetric Reactions
10.3.1 Uterine Cramping
Uterine cramping is integral to how misoprostol works in many obstetric uses. However, severe, continuous, or unusually painful contractions can be a warning sign of hyperstimulation or impending complications and must be promptly assessed.
10.3.2 Vaginal Bleeding
Vaginal bleeding is expected in indications such as miscarriage management or medical abortion. Nevertheless, excessive bleeding—such as soaking pads very rapidly, passing large clots repeatedly, or feeling faint—requires urgent medical attention.
10.4 Systemic Reactions
10.4.1 Fever and Chills
Patients may experience transient low-grade fever and chills following misoprostol administration. While this can be a benign pharmacologic effect, persistent high fever, rigors, or systemic symptoms can also signal infection and should not be ignored.
10.4.2 Headache and Dizziness
Headache, light-headedness, and dizziness may occur. People should avoid activities requiring full alertness, such as driving or operating machinery, if they feel unwell or unstable.
10.5 Severe or Rare Side Effects
10.5.1 Uterine Rupture
Although rare, uterine rupture is a serious complication, particularly in women with prior uterine surgery or when misoprostol is used inappropriately. Symptoms may include sudden intense pain, cessation of contractions, abnormal bleeding, or signs of shock, and require immediate emergency intervention.
10.5.2 Sepsis
Systemic infection and sepsis can occur if retained tissue, contaminated procedures, or pre-existing infection go unrecognized. High fever, tachycardia, confusion, or feeling acutely ill after misoprostol use must prompt urgent evaluation.
10.5.3 Hemorrhage
Severe hemorrhage is a medical emergency. Misoprostol, while often used to control bleeding, can also be associated with heavy blood loss in certain contexts. Any suspicion of uncontrolled hemorrhage necessitates immediate hospital care, potential transfusion, and expert management.
11. Common Side Effects
11.1 Mild Gastrointestinal Upset
Mild gastrointestinal disturbance is frequently observed. Many individuals describe transient discomfort that appears shortly after administration. This may include:
- Slight queasiness
- A fleeting sense of digestive imbalance
These symptoms generally resolve spontaneously and typically do not require intervention.
11.2 Transient Abdominal Pain
Short episodes of abdominal aching may occur due to prostaglandin-mediated smooth-muscle activation. The discomfort is usually mild, rhythmic, and self-limiting. Rest, hydration, and calm breathing may ease the sensation.
11.3 Vaginal Spotting or Cramping
Some users experience minimal spotting or localized pelvic cramping. This reaction often reflects the medication’s influence on uterine receptors. While generally benign, persistent or heavy bleeding warrants professional evaluation.
11.4 Mild Fever and Chills
A modest rise in body temperature may occur temporarily. Occasional chills, warmth, or generalized malaise can accompany this response. These manifestations are usually short-lived and do not indicate infection.
11.5 Headache and Fatigue
Headaches, light pressure sensations, or fatigue may appear. These reactions tend to be mild and brief. Hydration, rest, and reduced sensory stimulation may provide relief.
12. Drug Interactions
12.1 Interaction With Other Uterotonics
Co-administration with other agents that stimulate uterine activity may amplify contractile effects. This may increase the likelihood of uterine hypertonicity. Clinical oversight is essential when combining medications with overlapping physiologic actions.
12.2 Interaction With NSAIDs and Gastroprotective Agents
Misoprostol is frequently paired with NSAIDs to protect gastric mucosa. However, certain NSAIDs may modify its therapeutic profile. Additional gastroprotective drugs—such as proton pump inhibitors—may influence its perceived efficacy but do not typically create harmful interactions.
12.3 Interaction During Medical Abortion Regimens
When used within clinical protocols involving other hormonal or prostaglandin-modulating medications, interactions may influence timing or intensity of physiologic responses. Oversight by qualified healthcare professionals is required.
12.4 Medications Increasing Bleeding Risk
Agents that alter coagulation—anticoagulants, antiplatelets, or herbal supplements like ginkgo—may increase bleeding tendencies. Risk–benefit assessment is important when such combinations are considered.
12.5 Alcohol and Tobacco Considerations
Alcohol may potentiate dehydration and exacerbate gastrointestinal effects. Tobacco use can affect mucosal healing and vascular responses. Limiting these substances may reduce adverse reactions.
13. Careful Administration
13.1 Patients With Cardiovascular Disorders
Individuals with cardiac fragility may experience hemodynamic sensitivity. Minor shifts in blood pressure or heart rate can occur. A cautious approach ensures patient safety.
13.2 Patients With Renal Impairment
Renal dysfunction can alter drug elimination pathways. Adjustments and observation may be required to prevent accumulation or intensified side effects.
13.3 Patients With Hepatic Impairment
As hepatic metabolism influences prostaglandin analog activity, those with hepatic insufficiency may respond unpredictably. Clinical monitoring is recommended.
13.4 History of Cesarean Section or Uterine Surgery
Individuals with uterine scarring may face heightened sensitivity to uterine-active agents. Hyperstimulation risk requires thoughtful clinical evaluation before use.
13.5 Patients With Severe Anemia
Users with reduced hemoglobin reserves should be monitored closely due to the potential for bleeding or exaggerated fatigue.
13.6 Patients With Gastrointestinal Diseases
Those with inflammatory bowel disorders or chronic gastrointestinal irritation may experience amplified digestive disturbances. Professional guidance helps minimize complications.
14. Special Populations
14.1 Administration to Elderly
Older adults may exhibit altered drug metabolism and heightened sensitivity. Gentle titration is often considered in clinical contexts.
14.1.1 Adjustments in Gastric Protection Therapy
Elderly individuals receiving NSAIDs for chronic conditions may rely on gastric protection. Misoprostol’s gastroprotective role is valuable, though dose adjustments may be required.
14.2 Administration to Pregnant Women
Misoprostol exerts potent uterotonic activity. Its use during pregnancy is restricted to specific, supervised medical indications. Unsupervised use poses significant risk.
14.2.1 Pregnancy Risks and Fetal Harm
Misoprostol may induce strong uterine contractions and fetal harm when used outside controlled settings. Medical oversight ensures safe and appropriate use.
14.2.2 Medical Abortion vs. Contraindicated Uses
In regulated healthcare environments, misoprostol may be used in combination protocols for pregnancy termination. Outside approved contexts, it is contraindicated due to substantial danger.
14.3 Administration to Nursing Mothers
Trace amounts of misoprostol metabolites may enter breast milk. While exposure is generally minimal, breastfeeding individuals should consult medical professionals.
14.3.1 Misoprostol in Breast Milk
Available evidence suggests low levels are present and typically transient. Monitoring infants for irritability or diarrhea may be advised.
14.4 Administration to Children
Pediatric use is rare and generally reserved for highly specific conditions under specialist supervision.
14.4.1 Limited Data and Safety Concerns
Long-term safety information in children is limited. Clinical prudence is necessary.
14.4.2 Pediatric Off-Label Use
In certain rare circumstances, specialists may consider off-label use, but only within hospital settings equipped for monitoring.
15. Overdosage
15.1 Clinical Manifestations of Overdose
Excessive dosing may provoke profound gastrointestinal symptoms, intense cramping, or severe systemic malaise. Early identification is crucial.
15.2 Gastrointestinal Toxicity
Pronounced diarrhea, dehydration, and electrolyte imbalance may occur. Medical stabilization is required to prevent complications.
15.3 Uterine Hyperstimulation and Hemorrhage
Overstimulation of uterine tissue can lead to dangerous hypertonicity or bleeding. This reaction demands urgent care.
15.4 Emergency Management Guidelines
Treatment focuses on supportive stabilization, fluid correction, symptomatic relief, and close monitoring in a controlled environment.
16. Handling and Safety Precautions
16.1 Proper Tablet Storage and Handling
Tablets should be protected from moisture and handled with clean, dry hands. Misoprostol is sensitive to environmental degradation.
16.2 Safety Precautions for Healthcare Providers
Gloves may be used when handling large quantities. Proper storage prevents accidental exposure.
16.3 Avoiding Accidental Exposure
Pregnant individuals should avoid unnecessary contact with crushed or broken tablets due to pharmacologic potency.
16.4 Disposal of Unused or Expired Medication
Disposal should follow local pharmaceutical regulations. Returning unused medication to a pharmacy or clinic is often advised.
17. Storage Requirements
17.1 Recommended Temperature
Store at controlled room temperature. Excessive heat may degrade potency.
17.2 Humidity and Light Protection
Blister packaging protects against humidity. Keep tablets away from direct light to maintain stability.
17.3 Shelf Life and Expiry
Misoprostol remains stable until the labeled expiration date if stored correctly. Extended exposure to air can shorten shelf life.
17.4 Storage During Travel
Use airtight containers and avoid storing near sources of heat. Consistent temperature preservation maintains medication reliability.






Popular Products




Similar Product