1. Introduction to Olvance M (Olmesartan/Metoprolol)
1.1 What is Olvance M?
Olvance M is a fixed-dose combination antihypertensive medication that integrates two pharmacologically distinct agents: olmesartan medoxomil and metoprolol. This dual-therapy formulation is designed to provide comprehensive cardiovascular regulation through complementary mechanisms.
- Olmesartan: Angiotensin II receptor blocker (ARB)
- Metoprolol: Beta-1 selective adrenergic blocker
- Indicated for patients requiring combination therapy for optimal blood pressure control
The medication is commonly prescribed when monotherapy proves insufficient or when a multidimensional approach to blood pressure management is clinically warranted.
1.2 Why Combination Therapy for Hypertension?
Hypertension is a multifactorial condition involving vascular resistance, neurohormonal activation, and sympathetic overactivity. Combination therapy addresses multiple pathophysiological pathways simultaneously.
- Dual-mechanism blood pressure reduction targeting RAAS and sympathetic systems
- Enhanced therapeutic efficacy compared to single-agent therapy
- Improved patient adherence through simplified dosing
- Reduction in long-term cardiovascular morbidity and mortality
This integrated strategy supports sustained hemodynamic stability and long-term vascular protection.
2. Composition and Formulation
2.1 Active Ingredients
Olvance M contains two well-established cardiovascular agents:
- Olmesartan medoxomil: A prodrug converted to olmesartan, which selectively blocks angiotensin II AT1 receptors.
- Metoprolol: A cardioselective beta-1 blocker that reduces heart rate and myocardial workload.
Together, these agents exert both vascular and cardiac effects, producing a balanced antihypertensive response.
2.2 Available Strengths and Dosage Forms
The medication is available in various strength combinations to accommodate individualized treatment requirements.
- Different dose ratios of olmesartan and metoprolol
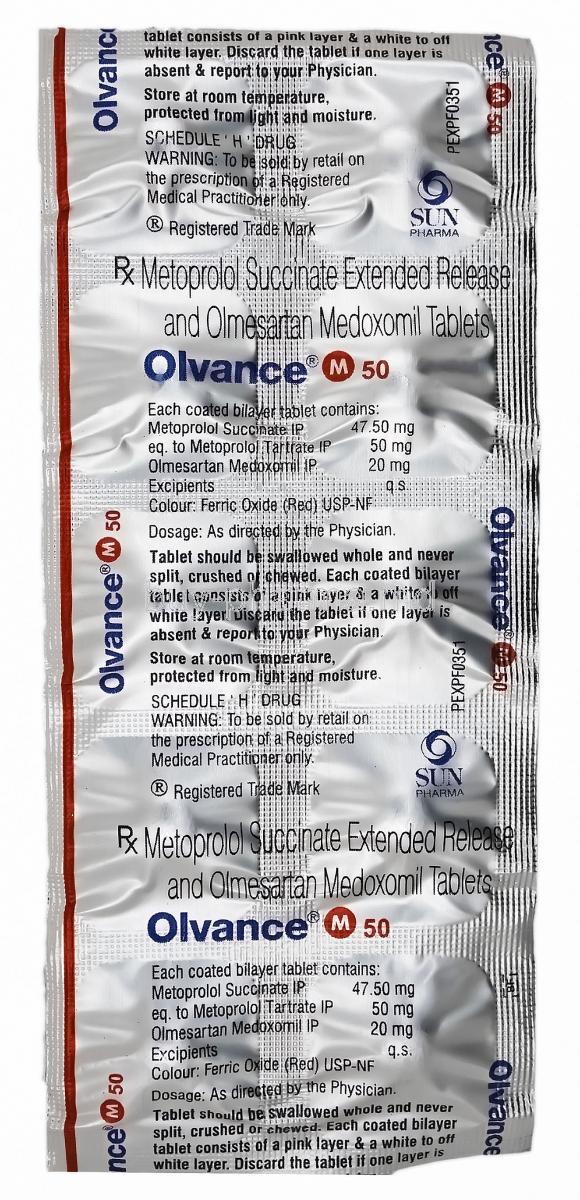
- Formulations may include immediate-release or extended-release metoprolol
- Dose selection based on clinical response and prior therapy
2.3 Excipients and Pharmaceutical Characteristics
In addition to active ingredients, Olvance M contains inert excipients that ensure stability and optimal drug delivery. Tablets are engineered to maintain consistent bioavailability and may incorporate controlled-release technology depending on formulation.
3. Mechanism of Action: How Olvance M Works
3.1 Mechanism of Olmesartan
Olmesartan antagonizes angiotensin II at the AT1 receptor, thereby interrupting a key vasoconstrictive and sodium-retentive pathway.
- Promotes vasodilation
- Reduces aldosterone secretion
- Decreases peripheral vascular resistance
3.2 Mechanism of Metoprolol
Metoprolol selectively inhibits beta-1 adrenergic receptors in cardiac tissue.
- Reduces heart rate and myocardial contractility
- Lowers cardiac output
- Decreases myocardial oxygen demand
3.3 Synergistic Effects of Combination Therapy
The combined inhibition of sympathetic stimulation and renin-angiotensin system activity produces a synergistic antihypertensive effect. This dual modulation enhances blood pressure control while offering additional cardioprotective benefits.
4. Approved Uses of Olvance M
4.1 Primary Indication
Olvance M is indicated for the management of essential hypertension, particularly in patients who require combination therapy to achieve target blood pressure levels.
- Treatment of moderate to severe hypertension
- Control of blood pressure in patients inadequately managed on single agents
4.2 Cardiovascular Risk Reduction
Effective blood pressure control reduces the risk of major cardiovascular events.
- Prevention of stroke
- Reduction in myocardial infarction risk
- Protection against long-term cardiac remodeling and heart failure progression
5. Off-Label Uses of Olmesartan/Metoprolol
5.1 Cardiovascular Off-Label Uses
- Stable coronary artery disease
- Post-myocardial infarction management
- Adjunct therapy in selected heart failure patients under specialist supervision
5.2 Arrhythmia and Rate Control
- Management of sinus tachycardia
- Heart rate control in atrial fibrillation (metoprolol component)
5.3 Other Potential Off-Label Applications
- Hypertension associated with anxiety or sympathetic hyperactivity
- Migraine prophylaxis
- Portal hypertension management in specialized settings
6. Dosage and Administration Guidelines
6.1 Recommended Starting Dose
The initial dose is determined based on prior antihypertensive therapy and patient-specific factors. Gradual titration allows optimization of efficacy while minimizing adverse effects.
6.2 Dose Adjustment
- Adjusted according to blood pressure response
- Modified based on tolerability and heart rate
- Transition from individual components may be considered
6.3 Administration Instructions
- May be taken with or without food
- Administer at the same time daily for consistent plasma levels
- Adherence is essential for sustained therapeutic benefit
6.4 Missed Dose and Discontinuation Guidance
If a dose is missed, it should be taken as soon as remembered unless it is close to the next scheduled dose. Abrupt discontinuation of the beta-blocker component may lead to rebound hypertension, tachycardia, or ischemic symptoms.
7. Side Effects of Olvance M
7.1 Common Side Effects
- Dizziness
- Fatigue or lethargy
- Bradycardia
- Hypotension
- Headache
- Mild gastrointestinal discomfort
7.2 Less Common but Clinically Significant Effects
- Cold hands and feet
- Sleep disturbances or vivid dreams
- Mood changes or depressive symptoms
7.3 Serious Adverse Reactions
- Severe hypotension or syncope
- Symptomatic bradycardia or heart block
- Acute kidney injury
- Hyperkalemia
- Rare angioedema
8. Drug Interactions
8.1 Antihypertensive and Cardiovascular Drug Interactions
- Other beta-blockers
- Non-dihydropyridine calcium channel blockers (e.g., verapamil, diltiazem)
- Diuretics and other RAAS inhibitors
8.2 Interactions Affecting Heart Rate and Conduction
- Digoxin
- Antiarrhythmic medications
8.3 Metabolic and Electrolyte Interactions
- Potassium supplements and potassium-sparing diuretics
- NSAIDs, which may reduce antihypertensive efficacy and impair renal function
8.4 CYP-Mediated Interactions (Metoprolol)
Metoprolol is metabolized via CYP2D6. Strong inhibitors such as certain antidepressants or antiarrhythmics may increase plasma concentrations and enhance beta-blockade.
9. Contraindications
9.1 Absolute Contraindications
- Hypersensitivity to olmesartan, metoprolol, or formulation components
- Severe bradycardia
- Second- or third-degree AV block without pacemaker
- Cardiogenic shock
9.2 RAAS-Related Contraindications
- Pregnancy
- Use with aliskiren in diabetic patients
9.3 Respiratory and Circulatory Contraindications
- Severe bronchial asthma
- Advanced peripheral arterial disease
10. Warnings and Important Precautions
10.1 Risk of Hypotension
Patients who are volume-depleted, elderly, or receiving high-dose diuretics may experience symptomatic hypotension, particularly during treatment initiation.
10.2 Renal Function Monitoring
Renal function should be assessed periodically, especially in patients with pre-existing kidney disease or conditions affecting renal perfusion.
10.3 Electrolyte Monitoring
Hyperkalemia may occur due to RAAS inhibition. Monitoring of serum potassium is recommended in high-risk individuals.
10.4 Risk of Bradycardia and Heart Block
Heart rate should be monitored, particularly in patients with conduction abnormalities or those receiving concomitant rate-lowering medications.
10.5 Abrupt Discontinuation Risk
Sudden withdrawal of the beta-blocker component may precipitate rebound hypertension, angina, or acute coronary events. Gradual dose tapering is advised.
11. Careful Administration (Use with Caution)
11.1 Patients with Renal or Hepatic Impairment
Patients with compromised renal or hepatic function require meticulous dose selection and ongoing clinical surveillance. Both components of Olvance M influence hemodynamic and metabolic processes that may be altered in organ dysfunction.
- Reduced renal perfusion may increase the risk of acute kidney injury, particularly in patients with renal artery stenosis or chronic kidney disease.
- Periodic monitoring of serum creatinine and electrolyte levels is recommended.
- In hepatic impairment, metabolism of metoprolol may be diminished, potentially leading to increased systemic exposure.
Therapy should be initiated cautiously. Gradual titration and close observation are essential to prevent excessive pharmacodynamic effects.
11.2 Patients with Diabetes Mellitus
Beta-blockers may obscure early adrenergic warning signs of hypoglycemia, such as tremor, palpitations, and tachycardia. This masking effect can delay recognition of dangerously low blood glucose levels.
- Patients should be educated to recognize non-adrenergic symptoms such as sweating, confusion, or dizziness.
- Regular glucose monitoring is strongly advised.
- Adjustments in antidiabetic therapy may be required.
Careful metabolic monitoring is particularly important in insulin-dependent individuals.
11.3 Patients with Thyroid Disorders
Metoprolol may attenuate clinical manifestations of hyperthyroidism by suppressing sympathetic symptoms. While this may provide symptomatic relief, it can also obscure disease progression.
- Masked symptoms may include tachycardia, tremor, and anxiety.
- Abrupt discontinuation in hyperthyroid patients may precipitate thyroid storm.
Gradual dose reduction and regular thyroid function assessment are recommended when clinically indicated.
11.4 Patients with Peripheral Vascular Disease or Raynaud’s Phenomenon
Beta-adrenergic blockade may exacerbate peripheral circulatory insufficiency by reducing cardiac output and peripheral perfusion.
- Worsening of intermittent claudication or cold extremities may occur.
- Symptoms of Raynaud’s phenomenon may intensify.
Clinical monitoring for peripheral ischemic symptoms should be performed throughout therapy.
12. Administration in Special Populations
12.1 Administration to Elderly Patients
Elderly patients often exhibit increased pharmacodynamic sensitivity and reduced physiological reserve. Age-related decline in renal and hepatic function may alter drug clearance.
- Initiate treatment at lower doses when appropriate.
- Titrate gradually based on blood pressure and heart rate response.
- Monitor for orthostatic hypotension, dizziness, and bradycardia.
Frequent clinical evaluation helps minimize the risk of falls and cardiovascular complications.
12.2 Administration During Pregnancy
Agents that act on the renin-angiotensin system, including olmesartan, carry a well-documented risk of fetal toxicity. Exposure during pregnancy may impair fetal renal development and lead to serious complications.
- Contraindicated, particularly during the second and third trimesters.
- Potential risks include oligohydramnios, fetal renal failure, pulmonary hypoplasia, and neonatal death.
If pregnancy is detected, the medication should be discontinued promptly and alternative therapy initiated.
12.3 Administration to Nursing Mothers
Both olmesartan and metoprolol may be excreted into breast milk in small quantities. Although clinical impact may be limited, potential exposure to the nursing infant should be considered.
- Assess the risk-benefit balance before prescribing.
- Monitor infants for signs of bradycardia, hypotension, or poor feeding if therapy is continued.
Clinical judgment should guide decisions regarding continuation of breastfeeding or medication.
12.4 Administration to Pediatric Patients
Safety and efficacy in pediatric populations have not been firmly established for this fixed-dose combination.
- Limited clinical data available.
- Use only under specialist supervision when considered necessary.
Dose individualization and careful monitoring are mandatory if therapy is initiated.
13. Overdose Management
13.1 Symptoms of Overdose
Excessive exposure to Olvance M may produce profound cardiovascular depression and systemic instability. Clinical manifestations may appear rapidly and require urgent medical intervention.
- Severe hypotension
- Marked bradycardia or atrioventricular block
- Cardiogenic shock
- Respiratory depression
- Altered mental status or syncope
The severity of symptoms depends on dose, patient comorbidities, and time to treatment.
13.2 Emergency Treatment and Supportive Care
Management focuses on rapid stabilization and supportive therapy.
- Early gastric decontamination in recent ingestion cases
- Intravenous fluids to restore hemodynamic stability
- Vasopressors for persistent hypotension
- Atropine for symptomatic bradycardia
- Glucagon for severe beta-blocker toxicity
- Continuous cardiac and hemodynamic monitoring
Advanced supportive care in a critical care setting may be required in severe cases.
14. Storage and Stability
14.1 Recommended Storage Conditions
Proper storage preserves drug potency and prevents degradation.
- Store at controlled room temperature
- Protect from excessive heat, moisture, and direct light
- Keep in a dry environment
Exposure to adverse environmental conditions may compromise product integrity.
14.2 Shelf Life and Packaging Integrity
The medication should be retained in its original packaging until use.
- Blister packs and sealed containers protect against humidity and contamination
- Do not use if packaging is damaged or expiration date has passed
Maintaining packaging integrity ensures stability throughout the product’s shelf life.
15. Handling Precautions and Patient Safety
15.1 Safe Handling and Dispensing Practices
Tablets should be handled carefully to preserve their release characteristics.
- Avoid crushing or splitting extended-release formulations
- Dispense only intact tablets unless otherwise directed
- Store out of reach of children
15.2 Patient Counseling Points
Patient education is essential for optimal therapeutic outcomes.
- Take the medication consistently at the same time each day
- Do not discontinue abruptly without medical advice
- Monitor blood pressure and pulse regularly
- Report symptoms such as dizziness, fainting, or unusually slow heartbeat
Adherence remains a cornerstone of effective long-term cardiovascular management.
15.3 Disposal Guidelines
Unused or expired medication should be disposed of responsibly.
- Do not flush tablets down the toilet or drain unless instructed
- Use authorized medication take-back programs when available
- If disposal at home is necessary, mix with undesirable substances and discard securely
16. Key Clinical Monitoring Parameters
16.1 Blood Pressure and Heart Rate Monitoring
Routine monitoring ensures therapeutic effectiveness and early detection of excessive pharmacologic effects.
- Regular blood pressure measurements
- Assessment of resting heart rate
- Evaluation for symptomatic hypotension or bradycardia
16.2 Renal Function and Electrolytes
Renal function tests and electrolyte assessments should be performed periodically, particularly in high-risk patients.
- Serum creatinine and estimated glomerular filtration rate
- Serum potassium levels
16.3 Signs of Adverse Cardiovascular Effects
Clinical evaluation should include assessment for potential complications.
- Worsening heart failure symptoms
- Peripheral edema or circulatory insufficiency
- Conduction abnormalities or arrhythmias
Early identification of adverse effects allows timely intervention and optimization of therapy.
Popular Products




Similar Product