Nivaquine P Suspension, Chloroquine
- Introduction
- Overview of Nivaquine P Suspension
- Therapeutic relevance of Chloroquine
- Overview of FDA/WHO guidance and global usage patterns
- Composition
- How It Works
- Uses
- Off-Label Uses
- Dosage and Administration
- Side Effects
- Common Side Effects
- Important Precautions
- Warning
- Contraindications
- Careful Administration
- Drug Interactions
- Administration to Elderly
- Administration to Pregnant Women and Nursing Mothers
- Administration to Children
- Overdosage
- Handling Precautions
- Storage
Introduction
Nivaquine P Suspension provides clinicians with a precisely calibrated liquid form of chloroquine, enabling accurate, patient-specific dosing against malaria. Leveraging the time-tested therapeutic efficacy of chloroquine—which not only attacks the parasite but also offers other benefits—the suspension remains highly relevant. It is a widely acknowledged, foundational treatment in endemic areas, indicated for both acute malaria episodes and prophylactic prevention, ensuring its continued necessity wherever malaria persists as a major public health burden.
Overview of Nivaquine P Suspension
Nivaquine P Suspension delivers a dose of chloroquine phosphate in a liquid form specifically created for easy oral use by both children and adults. The formulation is optimized with specific viscosity and $\text{pH}$ levels, along with high dispersibility, which simplifies administration while ensuring effective drug absorption (favorable pharmacokinetic profile). Extensive clinical data confirms that the suspension remains stable across various environmental conditions, making it particularly reliable for deployment in remote or resource-limited settings.
Therapeutic relevance of Chloroquine
Despite evolving drug resistance, Chloroquine remains a cornerstone drug, primarily valued for its ability to effectively halt the malaria parasite during its growth phase. Its usefulness extends far beyond malaria, however, due to its immunological effects, which are leveraged in treating autoimmune disorders like rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) by modulating cytokine signaling to relieve symptoms. Chloroquine's track record of inhibiting parasites at the crucial stage, dialing down inflammatory mediators, and its extensive clinical history continue to inspire ongoing medical research and discovery.

Overview of FDA/WHO guidance and global usage patterns
Global health agencies strictly govern the use of chloroquine-based treatments. The World Health Organization (WHO) establishes specific treatment regimens, outlines contraindications, and provides guidelines for monitoring resistance, especially where Plasmodium falciparum resistance is established. Concurrently, agencies like the FDA ensure treatment quality through mandates on quality assurance, active pharmacovigilance, and strict manufacturing standards.
These harmonized international frameworks guide global usage patterns: utilization is higher in areas dominated by P. Vivax and P. Ovale, while reliance is decreased in zones known for resistance. Nevertheless, chloroquine remains deployed for specific, approved non-malarial indications. Adherence to these unified standards is crucial for promoting evidence-based applications worldwide.
Composition
Active ingredient: Chloroquine phosphate
Chloroquine phosphate is the workhorse of the medication delivering an strike by threading itself into the parasite’s cellular machinery with surgical precision. Its knack, for dissolving in water and its ready absorption make it an ideal choice, for suspension blends that demand a spread.
Inactive excipients and formulation characteristics
The suspension contains essential excipients—inactive ingredients—that serve specific functional roles to ensure the medicine is effective and user-friendly. These include suspending agents which stabilize the mixture, flavoring additives designed to improve taste and encourage patients (especially children) to take the full dose (boost compliance), and preservatives that maintain product integrity throughout its shelf life. The inclusion of these components results in a drug profile that guarantees stable and reliable therapeutic delivery.
Physical properties and shelf-life indicators
Nivaquine P Suspension is consistently recognizable by its defining characteristics: a certain opacity (cloudiness), a uniform distribution of particles, and its unique color. The product's shelf-life is critically dependent on its tolerance for temperature changes, the stability of the inactive ingredients (excipients), and the integrity of the container and closure system. Early signs of degradation, such as the formation of a separate layer or a distinct change in viscosity (thickness), often serve as flags that the medication is starting to break down.
How It Works
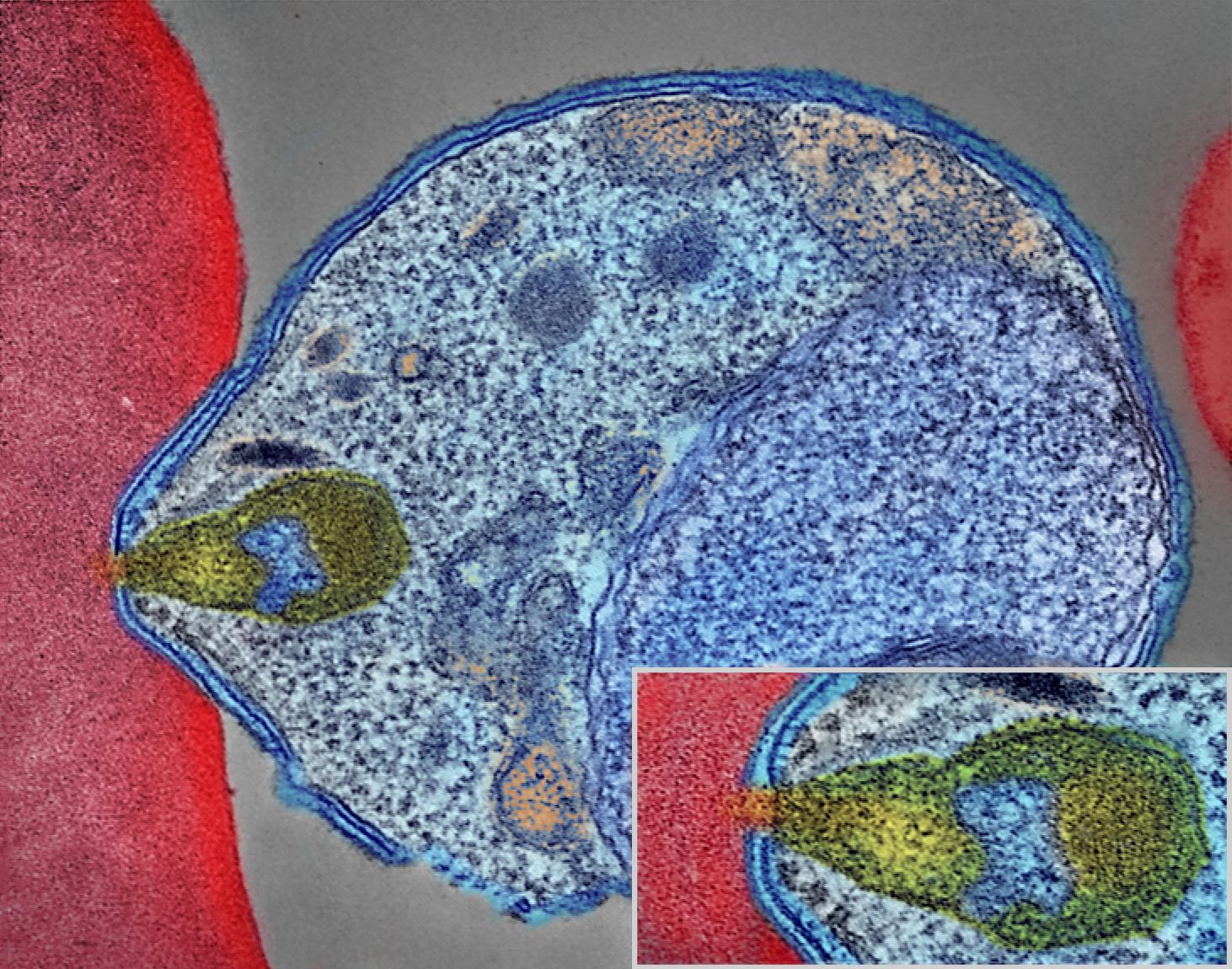
Mechanism of action in malaria parasites
Chloroquine kills the malaria parasite by interfering with its ability to detoxify the breakdown product of hemoglobin, known as heme. Normally, the parasite converts toxic heme into a harmless crystal called hemozoin inside its food vacuole. By blocking this conversion, chloroquine causes toxic, free heme to accumulate. This excess heme damages the parasite's internal membranes, leading to cell disruption and, ultimately, the parasite's death.

Immunomodulatory effects in autoimmune diseases
Chloroquine has subtle but significant immunological effects, primarily by dampening the signaling of Toll-like receptors (TLRs). This action reduces the immune system's efficiency at presenting foreign material (antigens) to other cells and decreases the release of inflammatory cytokines. Although its overall immune impact is modest, it subtly influences the course of immune activity throughout the body without broadly impairing general immune function.
Cellular and biochemical pathways influenced
Chloroquine initiates several key cellular effects: it interferes with the acidification of lysosomes, disrupts various cellular signaling pathways, and modifies the movement of calcium within cells. These widespread downstream effects alter the cell's internal balance (equilibrium), subtly influencing both the survival of pathogens and the host's immune response. Researchers continue to study the complex way these interconnected pathways contribute to chloroquine's overall profile in modern science.
Uses
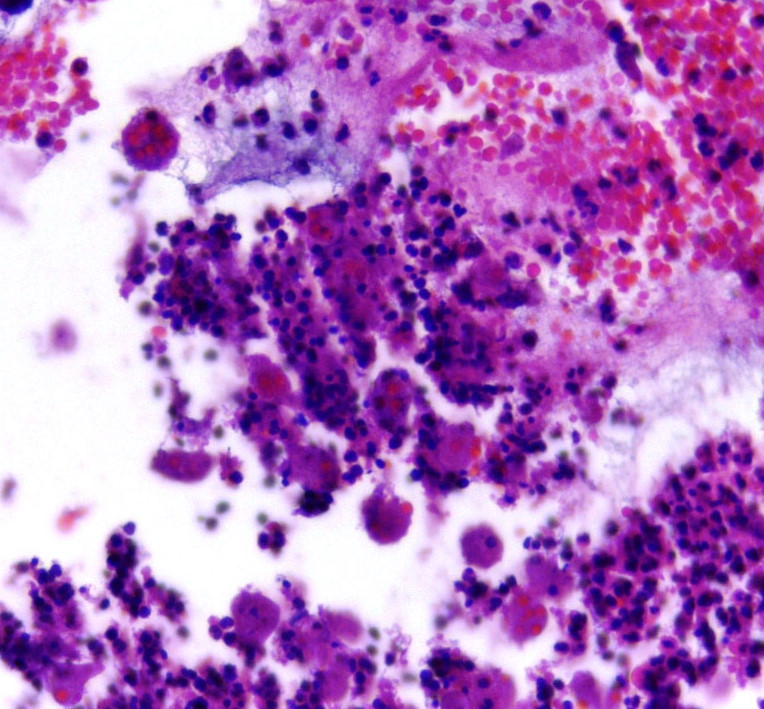
Treatment of malaria (Plasmodium vivax, P. ovale, P. malariae)
Chloroquine remains a fundamental part of the treatment strategy for malaria caused by the parasites Plasmodium vivax, P. Ovale, and P. Malariae. Quick treatment interventions are effective at immediately stopping the parasites from multiplying, while a sustained course of the drug ensures complete eradication. The primary benefits of using chloroquine include interrupting parasite replication in the red blood cells, resulting in a rapid drop in parasite load, and fewer fever episodes. Due to its consistent effectiveness in areas where drug resistance is not yet common, chloroquine holds its place as a reliable, established antimalarial treatment.
Treatment of rheumatoid arthritis
In the treatment of rheumatoid arthritis (RA), chloroquine demonstrates multiple immune-modulating effects. It alleviates inflammation by reducing the excessive release of inflammatory cytokines, which helps soothe joint pain and increase joint mobility. When used over time, chloroquine can significantly temper the autoimmune overreaction, leading to marked long-term improvements in functional outcomes. Compared to more aggressive disease-modifying agents, it generally exhibits a favorable tolerability profile, offering reliable relief amidst fluctuating inflammation.
Treatment of lupus erythematosus
In treating lupus erythematosus (SLE), chloroquine helps rebalance immune signaling, which effectively dampens the over-production of harmful autoantibodies. While its power is often concisely stated, detailed analysis shows its influence touches the skin, musculoskeletal system, and overall systemic disease manifestations. Patients frequently experience better maintenance of stability during flare-ups and better long-term control of the disease, leading to a more stable overall systemic balance (homeostasis) over time. Sustaining this therapeutic equilibrium is crucial for the long-term management of lupus.
Prophylaxis of malaria
When taken before exposure, chloroquine acts as an effective preventative (prophylactic) measure against malaria for both travelers and residents in endemic areas. It works by maintaining therapeutic levels of the drug in the bloodstream, creating an environment that is hostile to invading parasites.
Key advantages of this prophylactic use include: stable drug absorption (pharmacokinetic patterns), which simplifies dosing; flexibility for individuals managing travel schedules; and an easy-to-tolerate dosing schedule, which improves patient adherence. In regions where resistance is not present, chloroquine’s preventive capacity remains critically important.
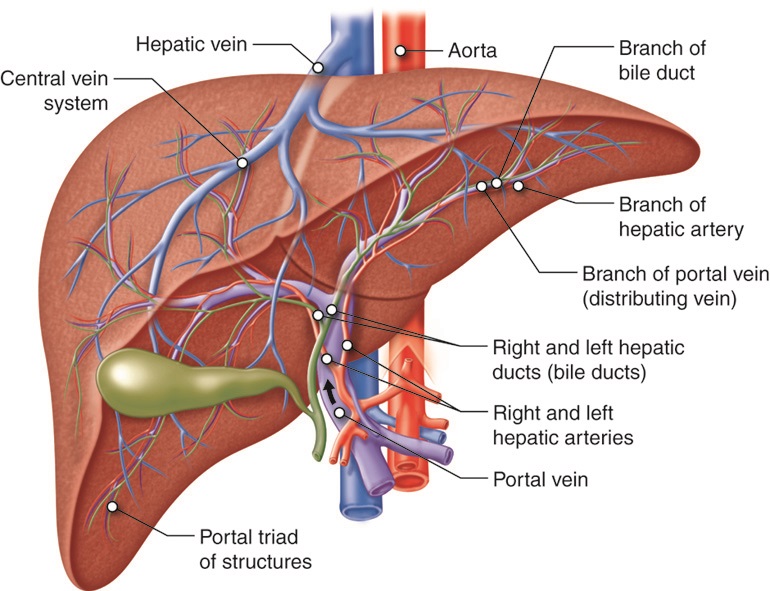
Use in extraintestinal amoebiasis
Chloroquine offers valuable supplementary treatment for extraintestinal amoebiasis, especially when the liver is involved (hepatic amebiasis), where its ability to penetrate deep tissues is necessary. At a cellular level, it quickly disrupts the viability of the ameba. This, combined with its wide tissue distribution, extends its therapeutic reach.
Clinical advantages of using chloroquine include:
- Improved penetration into liver tissues (hepatic parenchyma).
- Adjunctive effectiveness when paired with drugs that clear amebas from the gut (luminal amebicides).
- Reduced risk of abscess-related complications (suppurative complications).
Its supporting role strengthens the overall, comprehensive management of invasive amebic disease.
Off-Label Uses
Exploratory research has revealed chloroquine's potential to interfere with pathways essential for viral replication. While its immediate biochemical effects are clear, longer studies suggest broader implications for fighting viruses. Specifically, the compound has been investigated for its ability to:
- Block viral entry by altering the pH of cellular compartments called endosomes.
- Interfere with the glycosylation (sugar modification) of proteins on the viral surface.
- Weaken intracellular trafficking mechanisms that viruses need to propagate (spread) within the cell.
Although this area remains under active investigation, chloroquine's complex influence on viral biology continues to attract significant scientific interest.
Use in chronic inflammatory conditions
Chloroquine can benefit individuals with chronic inflammatory disorders by tempering exaggerated immune signaling. It subtly modifies how immune cells (leukocytes) respond, which results in a reduction of the overall inflammatory cascade. Clinical evidence suggests it helps alleviate persistent joint irritation (synovial irritation), low-grade inflammation throughout the body, and recurrent flare-ups caused by disordered immune pathways. While not a cure, this immunological recalibration contributes significantly to stable, long-term symptomatic management.
Potential role in porphyria cutanea tarda
Evidence indicates that chloroquine can be used as an adjunctive treatment for Porphyria Cutanea Tarda (PCT) by subtly modifying how porphyrins accumulate in the liver. A short course of treatment can help flush out excess porphyrins, and careful dosing is essential to avoid liver toxicity (hepatotoxicity).
The clinical benefits often include:
- A slow and steady reduction of the porphyrin burden.
- Alleviation of photosensitivity symptoms (skin reactions to light).
- Support for the liver’s natural detoxification pathways.
Because its effectiveness varies by patient, its use requires careful individualized clinical judgment.
Use in sarcoidosis management
In treating sarcoidosis, chloroquine's immune-modulating capability may help to reduce inflammation. Its immediate effects combine to lower the overall severity of the disease's multisystem involvement.
Chloroquine can be considered when standard treatments are ineffective or poorly tolerated, offering specific benefits such as:
- Reducing the quantity and size of lesions (diminishing the lesion burden).
- Helping regulate inflammatory mediators.
- Improving the capacity to control disease activity.
Due to these influences, it can serve as a viable alternative within a comprehensive management strategy for sarcoidosis.

Dosage and Administration
Recommended dosage for malaria treatment
The therapeutic dosing strategy for malaria treatment is designed to quickly reach drug concentrations high enough to kill the parasite, and then maintain sufficient levels in the blood for several days. This often involves a short, initial loading dose followed by smaller, tapered doses to ensure the complete elimination of the infection.
Key factors guiding this regimen are:
- Calculations based on patient weight to ensure precise dosing.
- Monitoring drug concentration in cases of severe disease.
- Strict adherence to set treatment intervals to minimize the risk of relapse.
Ultimately, this structure ensures the effective suppression of parasites in the blood (erythrocytic parasitemia) and provides rapid symptom relief.
Dosage for malaria prophylaxis
Prophylactic (preventive) dosing is typically lower than treatment doses and is taken at regular weekly intervals. This schedule maintains stable drug concentrations that are high enough to prevent the parasite's early development after a person is exposed.
A typical regimen involves:
- Starting the medication one to two weeks before entering a malaria-endemic area.
- Continuing use for the entire duration of exposure.
- Taking doses after leaving the area to eliminate any latent parasitic forms.
This consistent administration ensures strong preventive effectiveness, regardless of the local disease prevalence.
Dosage for autoimmune disorders
For non-malarial diseases, the prescribed dosage is designed to subtly modulate the immune system rather than deliver a quick, parasite-killing effect. Lower daily doses are used to influence immune signaling while prioritizing good patient tolerability gently.
This strategy aims to promote:
- Reduced levels of inflammation.
- Long-lasting reduction in disease symptoms.
- An effective approach for managing chronic diseases over the long term.
- Clinical improvement typically develops gradually, usually becoming noticeable only after several weeks of continuous treatment.
Pediatric dosing considerations
When prescribing chloroquine for children, clinicians must calculate the dosage precisely based on the child's weight to balance the need for effective treatment with the risk of toxicity. The liquid suspension formulation is particularly useful as it allows for an accurate dose, which is helpful for younger children whose ability to swallow pills may be inconsistent. Important considerations include:
- Adjusting the milligram-per-kilogram mg/kg dosage to account for the child's age and developing metabolism.
- Vigilantly monitoring for any signs of intolerance or adverse reactions.
- Ensuring the medication is administered consistently according to the established schedule.
By following these safety precautions, clinicians maintain both the effectiveness and safety of the treatment across the pediatric population.
Adjustments for hepatic or renal impairment
Patients who have impaired liver or kidney function require careful dose adjustments because their ability to process (metabolize) and remove (clear) drugs from the body is altered. A slight reduction in dosage may be sufficient for mild impairment, but severe dysfunction necessitates a much more significant adjustment.
These adjustments are intended to:
- Prevent the accumulation of the drug, thus avoiding toxicity.
- Keep drug concentrations within the optimal therapeutic window to avoid excessive levels.
- Align dosing intervals with the patient's slowed drug clearance rates.
From the initial dose change through subsequent follow-up, continuous and vigilant clinical monitoring is absolutely essential for these patients.
Correct administration technique for suspension formulations
Proper handling of the suspension formulation is critical to ensure accurate dosing. The bottle must be vigorously shaken before each use to ensure that the solid particles are evenly distributed (resuspended) throughout the liquid.
Achieving the correct technique involves:
- Using meticulously calibrated measuring instruments (e.g., dosing spoons or cups provided with the medication).
- Avoiding common household utensils like kitchen spoons, as their volume is highly imprecise and inconsistent.
- Consuming the dose immediately after measuring, as the particles will quickly settle and form sediment again.
Following these steps guarantees that the intended therapeutic dose is delivered consistently.
Side Effects
Overview of possible adverse effects
Adverse effects from the drug can manifest with varying signs and frequency, typically impacting the nervous, digestive, and visual systems. Patients may experience everything from temporary irritations to long-term toxicities that gradually accumulate with prolonged use. Clinicians must thoroughly understand these potential variations in order to provide sensible and effective patient management.
Short-term side effects
During the initial days of treatment, patients commonly experience short-term reactions. These effects are typically mild and tend to resolve on their own as the body adjusts to the medication.
The early side effects often observed include:
- Mild stomach upset (gastrointestinal distress).
- A temporary feeling of dizziness or imbalance.
- Increased skin sensitivity (e.g., photosensitivity or minor rash).
The severity of these early manifestations usually remains at a manageable level.
Long-term side effects
Prolonged use of the drug can lead to serious toxic reactions. These issues result from the cumulative effects of the drug and from the way it affects sensitive tissues, particularly over time.
Potential long-term concerns include:
- Changes in the retina that can impact vision (acuity).
- Weakness in the muscle system (myopathy).
- A condition where the skin becomes unusually dark due to pigment accumulation.
Consistent, ongoing long-term monitoring is essential to help reduce the risk of these complications.
Common Side Effects
Gastrointestinal disturbances
Discomfort related to the digestive system is among the most frequently reported side effects. Common signs include nausea, stomach pain, or alterations in bowel movements.
In most instances, these reactions lessen when the medication is taken with food or when the dosage is slightly adjusted. Although typically mild and temporary (fleeting dyspepsia), stomach upset can occasionally escalate into true drug intolerance if not addressed.
Headache and dizziness
Neurologic symptoms, commonly including headaches and dizziness, stem from temporary disruptions in the central nervous system's signaling. These effects can appear suddenly but usually lessen as the body adjusts to the medication.
Patients might experience:
- Lightheadedness that occurs early in the dosing regimen.
- Head pain that throbs or pulses rhythmically.
- Occasionally, a slight feeling of being off-balance or a faint blurring of vision may occur.
Maintaining good hydration and adhering to a consistent dosing routine typically helps manage and control these reactions.

Skin reactions
The skin's reaction to the medication can range from a mild symptom, like itching, to a more extensive, widespread rash. While brief, temporary eruptions might occur soon after starting the drug, long-term use can sometimes cause changes in skin color (pigmentation shifts). Furthermore, the drug can increase photosensitivity (making the skin more sensitive to sunlight), which worsens these skin issues. Reducing sun exposure is an important step to help prevent these reactions from flaring up.
Visual disturbances
Although visual disturbances are not common, they require careful monitoring. These issues can present as difficulty seeing clearly, trouble keeping things in focus, or subtle changes in how colors are perceived.
Potential causes include:
- The drug accumulates in the retinal tissue over time.
- Altered functioning of the eye's light-sensitive cells (photoreceptors).
- Fluctuations in the eye's ability to adjust focus (accommodation responses).
Early detection of these problems is crucial because it allows for intervention before permanent eye damage occurs.
Important Precautions
Need for ophthalmologic monitoring
Regular eye exams are a crucial safety precaution when patients are on long-term medication. While a quick assessment can detect immediate changes, extended follow-up is necessary to find damage that develops slowly over time.
To minimize the risk of toxicity, clinicians typically recommend:
- A complete baseline ocular assessment before starting any long-term therapy.
- Periodic reassessments of visual acuity (sharpness), visual fields, and color discrimination.
- Using advanced diagnostic tools, such as Optical Coherence Tomography (OCT) and fundus imaging, when the clinical situation requires it.
Monitoring the retina through these check-ups allows for early detection of changes, providing time to adjust the treatment plan and prevent permanent eye damage.
Risks of prolonged therapy
Extended exposure to chloroquine can lead to a buildup of toxicity, which eventually causes damage to organ systems. While short treatment courses are generally well-tolerated, the risk of serious side effects (amplified pharmacodynamic effects) increases significantly with the duration of therapy.
The key hazards associated with long-term use include:
- Progressive retinal damage that can ultimately lead to permanent vision loss.
- Electrical conduction problems in the heart muscle (cardiotoxicity).
- Persistent drug accumulation in tissues, linked to generalized weakness and muscle disease (myopathy).
Therefore, it is essential for clinicians to carefully weigh the potential risks against the anticipated benefits before committing a patient to a long-term treatment plan.
Precautions for hepatic disease
Liver impairment can significantly alter how chloroquine is processed and eliminated by the body. Even a slight increase in dosage can lead to a surge in drug exposure, increasing the risk of toxicity.
Therefore, precautionary measures should include:
- Starting therapy with a reduced dose for patients with moderate to severe liver impairment.
- Regularly monitoring liver function tests to detect early signs of liver toxicity (hepatotoxicity).
- Avoiding other liver-damaging agents (hepatotoxic agents) whenever possible.
Adopting these strategies helps reduce the risk of drug accumulation and subsequent damage to liver cells.
Precautions in glucose-6-phosphate dehydrogenase deficiency
Glucose-6-phosphate dehydrogenase (G6PD) deficiency renders patients susceptible to oxidative hemolysis (red blood cell destruction) upon drug exposure. Despite chloroquine having a comparatively lower risk of inducing these crises than other medications, prudent clinical practice and continuous vigilance are essential. To protect at-risk individuals and maintain their hematologic balance, healthcare providers must employ key preventative measures: these include screening for G6PD deficiency in high-prevalence areas prior to beginning any treatment, monitoring closely for signs of hemolysis such as jaundice, dark-colored urine, or a sudden drop in red blood cell count, and immediately discontinuing the therapy if hemolytic markers begin to worsen.
Warning
Severe toxicity risk with incorrect dosing
Chloroquine has a narrow therapeutic window, meaning there is only a small difference between an effective dose and a toxic dose, a margin that is even smaller in children. Even a slight miscalculation in dosing can lead to fatal poisoning (lethal intoxication).In cases of severe overdose, the clinical presentation may involve:
- Sudden and rapid collapse of the heart and circulatory system (cardiac and circulatory shutdown).
- Severe potassium depletion (hypokalemia) accompanied by dangerously low blood pressure (hypotension) that resists treatment.
- Seizures, coma, and respiratory arrest.
To prevent accidents, precise dosing and ensuring the medication is kept strictly out of reach of children are absolutely essential.
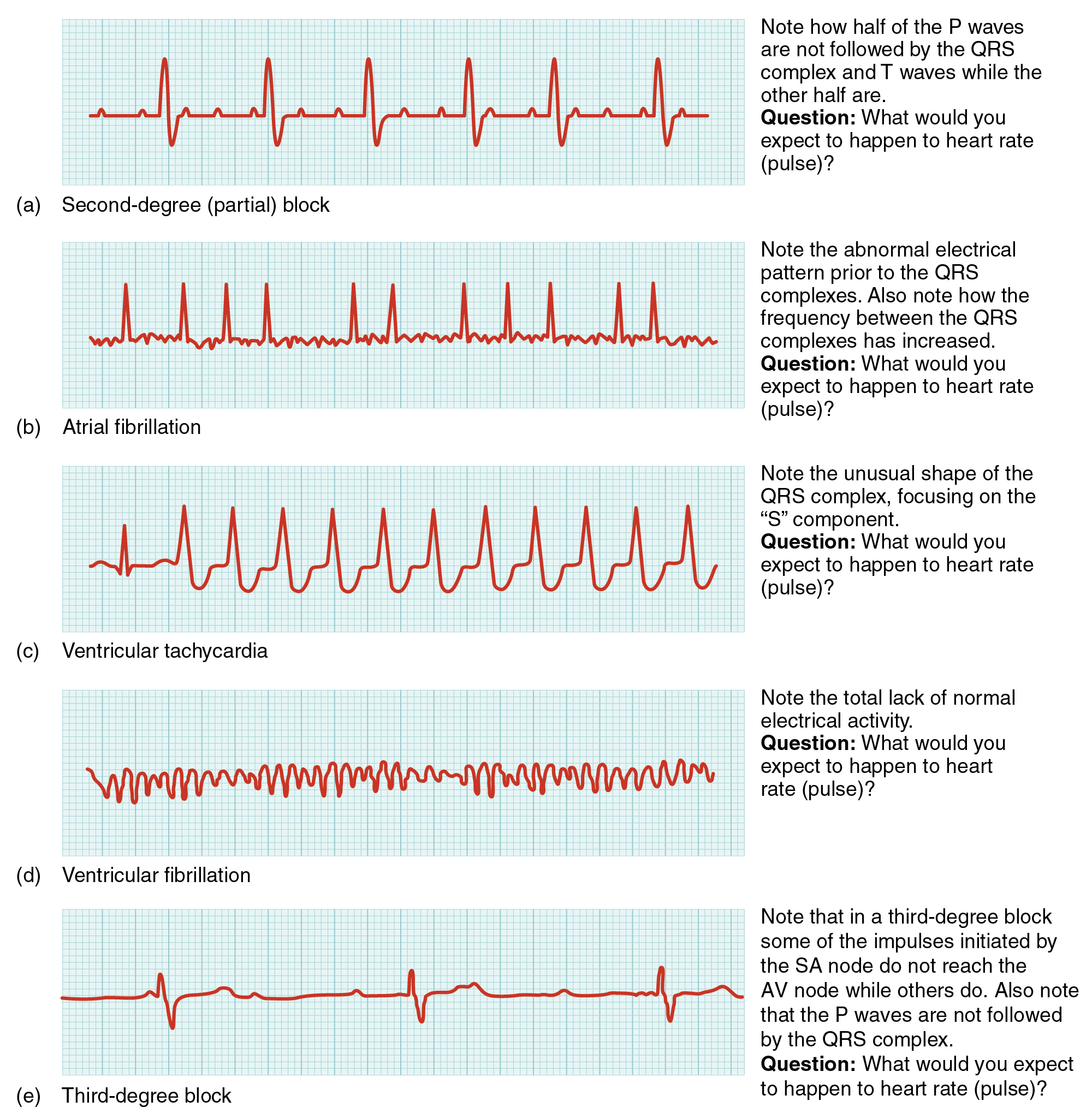
Cardiotoxicity warning and QT prolongation
Chloroquine can significantly affect heart function, often leading to a prolongation of the QT interval on an electrocardiogram. This risk is amplified if the patient is taking other QT-prolonging drugs or has a pre-existing heart condition. Key concerns related to this effect include:
- An increased risk of experiencing Torsades de Pointes—a serious, rapid, and irregular heart rhythm—and other cardiac arrhythmias.
- Potential abnormalities in the heart's electrical conduction, such as a heart block.
- The need for extra caution when treating patients with existing heart disease or electrolyte imbalances (like low potassium).
For high-risk patients or when higher doses are administered, continuous electrocardiographic (ECG) monitoring should be an integral part of their management plan.
Neurological complications
Neurotoxicity is another potential adverse reaction associated with chloroquine. Symptoms typically begin with changes in thinking and awareness (cognition), but in severe cases, they can escalate into full neurological crises.
Reported complications include:
- Persistent headaches, mental confusion, and increased irritability.
- Seizures and status epilepticus (prolonged seizures) in serious cases.
- Peripheral myopathy (weakness and damage to muscles) often appearing with extended therapy.
A prompt evaluation of any new neurological signs is crucial to prevent the issue from worsening into lasting damage.
Risk of irreversible retinal damage
Chloroquine-associated retinopathy often progresses without being noticed, and once it becomes advanced, the resulting vision loss can be permanent.
A brief episode of visual disturbance may signal the start of lasting damage, especially if exposure to the medication continues.
Typical signs of toxicity may include:
- Paracentral visual changes, such as difficulty reading small print.
- A bull’s-eye pattern seen on fundoscopic exam.
- Gradual worsening of central vision if the drug is not discontinued.
Early recognition of these warning signs and promptly stopping the medication are crucial for protecting any remaining vision.
Contraindications
Known hypersensitivity to chloroquine compounds
If a patient’s record shows a verified allergy to chloroquine or any related 4-aminoquinoline drugs, the medication should not be used.
Re-exposure to the substance can provoke an immune response.
Possible reactions may include:

- Respiratory symptoms, such as reduced breathing capacity.
- Severe, potentially life-threatening events requiring urgent care.
When this type of hypersensitivity appears, it is critical to choose an alternative treatment path.
Pre-existing retinal disorders
When chloroquine is used in someone who already has an underlying eye condition, the risk of vision loss increases significantly.
If an undiagnosed disorder is present, it may conceal early signs of toxicity and make the retina more vulnerable.
Situations where avoiding the drug is advisable include:
- Macular or other degenerative retinal diseases.
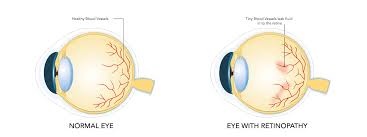
- Diabetic retinopathy, where the retinal microvasculature is already impaired.
- Inherited retinal dystrophies.
For affected individuals, the potential for harm generally far outweighs any possible benefit.
Patients with psoriasis
Chloroquine can aggravate psoriasis, leading to thicker plaques and, in some cases, triggering a particular subtype of the disease.
Even brief exposure may occasionally provoke a flare in predisposed people.
Key clinical points include:
- A noticeable increase in the severity of plaque lesions.
- The potential to precipitate erythrodermic psoriasis.
- Difficulty stabilizing the condition after a flare occurs.
For these reasons, clinicians typically avoid prescribing chloroquine to patients with current or past psoriasis unless no suitable alternative is available.
Porphyria contraindication
Individuals with porphyria should avoid chloroquine, as it can disrupt the body’s heme-production pathway and may trigger an acute episode.
Even minimal exposure can provoke symptoms in highly sensitive patients.
Possible outcomes include:
- Severe abdominal pain associated with acute crises.
- Autonomic instability often presents as rapid heart rate and elevated blood pressure.

- Neuropathy can lead to reduced muscle strength.
Avoiding chloroquine in all forms of porphyria is essential, as it carries a significant risk of provoking disease flare-ups.
Careful Administration
Patients with liver disease
In patients with impaired liver function, clinicians must adjust the dose carefully because reduced metabolic clearance alters how the drug is handled by the body.
Even brief fluctuations in hepatic activity can raise systemic drug levels, increasing the likelihood of toxicity.
Practical monitoring should focus on:
- Lowering the dosage to prevent overwhelming the liver’s metabolic capacity.
- Performing periodic liver function tests to detect signs of stress.
- Avoiding the medication altogether when a safer alternative exists.
These careful adjustments help maintain therapeutic benefits while minimizing strain on the liver.
Patients with renal impairment
When the kidneys aren’t functioning properly, they clear the drug more slowly, causing it to accumulate in both the bloodstream and within cells.
Short treatment courses may require minor adjustments, while long-term therapy often needs more significant dose recalibration.
Key considerations include:
- Modifying the dosage based on the kidneys’ filtration ability.
- Monitoring for early signs of ocular toxicity.
- Adjusting the interval between doses according to current renal performance.
These measures help ensure the drug’s behavior in the body remains safe and predictable despite impaired kidney function.
Patients with neurological disorders
Neurological conditions can heighten a person’s vulnerability to developing adverse symptoms.
Even a slight disruption in nervous system function may sharply increase sensitivity.
Recommended precautions include:
- Assessing neurological stability before initiating therapy.
- Monitoring for any emerging motor abnormalities.
- Avoiding concurrent use of medications known to lower the seizure threshold.
With these measures in place, the overall integrity of the nervous system can be maintained throughout treatment.
Immunocompromised patients
When the immune system is weakened, patients often show altered immune responses and become more prone to infections.
Even brief periods of immune instability can gradually lead to complications.
Effective clinical management may include:
- Close monitoring for signs of infection.
- Cautious evaluation of treatment effects along with any associated side effects.
- Collaborating with specialists who oversee the underlying immune disorder.
Maintaining therapeutic effectiveness while preserving overall stability is essential for these individuals.
Drug Interactions
Interaction with antacids
Magnesium- or aluminum-based antacids can interfere with gastrointestinal absorption by forming complexes that reduce drug uptake.
This can quickly diminish circulating levels.
To lessen the impact of this interaction:
- Separate doses by two to four hours.
- Monitor for reduced effectiveness, particularly in malaria treatment or autoimmune flare control.
- Consider alternative acid-reducing therapies if needed.
With proper timing, the medication’s bioavailability is maintained and its therapeutic effect remains intact.
Interaction with cardiac medications
When cardiac medications that influence electrical conduction are used together, their electrophysiologic effects can amplify one another.
A minor disturbance in heart rhythm can escalate into a more significant arrhythmia.
Clinicians should exercise caution with:
- Beta-blockers or calcium-channel blockers slow the passage of electrical signals through the heart.
- Antiarrhythmic agents are known to prolong the QT interval.
- Any coexisting cardiac disease.
Because this combination can shift the balance toward instability, careful monitoring is essential.
Interaction with antiepileptic drugs
Certain antiepileptic drugs can lower the seizure threshold, modify enzyme activity, and ultimately change the medication’s pharmacokinetics.
Even a subtle, almost unnoticed imbalance may lead to a breakthrough seizure.
Key concerns include:
- Reduced effectiveness of antiepileptic agents when they compete for metabolic pathways.
- A heightened risk of neurotoxicity.
- The need to adjust the dose of whichever medication is being used.
When these drugs are combined, close monitoring of neurological function becomes essential.
Interaction with antibiotics
Some antibiotics—particularly macrolides and fluoroquinolones—can increase the risk of cardiotoxic effects.
This becomes especially significant when both medications influence cardiac repolarization.
Possible outcomes include:
- More pronounced QT-interval prolongation.
- A higher risk of developing torsades de pointes.
- Pharmacodynamic interactions that intensify these effects.
Because of these risks, clinicians should use extra caution when prescribing these drugs together.
Risk of additive QT prolongation
When multiple QT-prolonging medications are used at the same time, their effects on cardiac conduction can compound.
Even small delays in repolarization can accumulate over time and eventually trigger arrhythmias.
Strategies to reduce this risk include:
- Obtaining a baseline ECG and repeating it at scheduled intervals.
- Correcting issues such as low potassium or magnesium levels.
- Avoiding combinations of QT-prolonging drugs whenever possible.
Consistent monitoring significantly lowers the likelihood of a cardiac event.
Administration to Elderly
Dosage considerations for geriatric patients
Because many older adults metabolize and excrete medications more slowly—both through the liver and kidneys—clinicians often choose lower, more conservative doses.
Even brief increases in drug levels can lead to adverse effects.
Dose adjustments may involve:
- Starting with a low initial dose and increasing it gradually through careful titration.
- Extending the interval between doses to prevent accumulation.
- Performing a thorough medication review to reduce the risks associated with polypharmacy.
These adjustments help widen the safety margin of treatments in the context of age-related physiological changes.
Increased risk of retinal and cardiac toxicity
Age-related degenerative changes make older adults particularly vulnerable to cardiac toxicity.
Early warning signs can escalate quickly if not addressed promptly.
Clinical concerns may include:
- Rapid onset of retinopathy.
- A higher tendency toward QT prolongation and arrhythmic events.
- Reduced physiological reserve, making it harder for the body to recover from adverse reactions.
Proactive, ongoing monitoring is essential for preventing these complications.
Monitoring requirements
Adhering to a structured monitoring plan is essential for protecting the health of older adults.
Regular check-ups help detect deviations from their physiological baseline early on.
Recommended oversight measures include:
- Consistent ophthalmology visits for eye examinations.
- Routine ECG assessments.
- Laboratory tests to evaluate liver and kidney function, as well as electrolyte levels.
This comprehensive monitoring approach enhances safety and supports successful treatment outcomes.
Administration to Pregnant Women and Nursing Mothers
Safety during pregnancy
Ensuring safety during pregnancy requires balancing the mother’s therapeutic needs against any potential risk to the developing fetus.
Despite uncertainties, some patients still require treatment, particularly in regions where vector-borne diseases pose an immediate threat.
Key factors influencing decision-making include:
- Thoroughly evaluating disease severity and the patient’s overall vulnerability.
- Reviewing possible alternative treatment options.
- Maintaining close supervision throughout therapy.
Any brief, short-term exposure should be justified within a carefully structured clinical framework.
Placental transfer and fetal risks
The drug can cross biological barriers and enter the fetal circulation at detectable levels.
Once it passes through the placenta, it may pose risks to the developing eyes, nervous system, and hematopoietic system.
Potential fetal concerns include:
- Accumulation of the compound in ocular tissues, leading to structural changes and altered function.
- Disruption of normal pathway development within the growing brain.
- Possible suppression of blood-cell production.
Accurate risk assessment must consider both gestational age and the mother’s total cumulative dose.
Breastfeeding considerations
Only small amounts of the medication pass into breast milk during breastfeeding.
Although these levels are generally low, they may still matter for infants whose metabolic systems are not fully developed.
Key points to consider when breastfeeding include:
- Determining whether the mother’s need for treatment outweighs the potential exposure to the infant.
- Monitoring how the medication is taken to help minimize peak concentrations in breast milk.
- Considering temporary interruption of breastfeeding if the risks become significant.
Close coordination with appropriate specialists is often highly beneficial.

Monitoring infants for potential side effects
Newborns exposed to the medication in utero or through breast milk should be monitored closely for any signs of toxicity.
Even a brief, subtle change can signal a developing problem if not addressed promptly.
Recommended areas of observation include:
- Scheduling ophthalmology evaluations to detect visual disturbances early.
- Tracking feeding behaviors, irritability, and sleep patterns.
- Screening for abnormalities in liver, kidney, or hematologic function.
Early detection helps ensure timely and effective intervention.
Administration to Children
Pediatric safety profile
Children differ in both how they respond to a medication and how they metabolize it, so safety standards must be tailored specifically for them.
Because their organs are still developing, they are often more sensitive to various effects.
Important considerations include:
- Carefully evaluating how tolerability varies across different ages.
- Adjusting the dose according to body weight and the maturity of the child’s metabolic systems.
- Quickly assessing any behavioral changes or emerging symptoms.
In pediatric patients, a cautious, conservative strategy helps keep complications to a minimum.
Dosing accuracy and measuring tools
When treating children, precise dosing is crucial—too little renders the medication ineffective, while too much can lead to toxicity.
Even small variations in measurement can meaningfully change how the drug behaves.
To maintain accuracy:
- Use calibrated syringes or other reliable measuring tools.
- Avoid household spoons, which create inconsistent dosing.
- Give caregivers clear instructions on correct measurement and administration.
An accurate dose protects the child and ensures the treatment works as intended.
Risk of overdose in children
Children are particularly vulnerable to drug accumulation because of their limited physiological reserves and rapid absorption rates.
Even small deviations from the recommended dose can trigger adverse effects.
Common signs of overdose may include:
- Abnormalities in cardiac conduction.
- Significant neurological symptoms, such as seizures.
- Gastrointestinal upset along with metabolic instability.
If an overdose is suspected, immediate medical assessment is crucial.

Need for parental supervision
Active participation from a parent or caregiver is essential to ensure medications are stored properly, given at the correct dose, and monitored carefully.
Even a brief lapse in attention can lead to accidental ingestion or missed doses.
Helpful supervisory practices include:
- Storing medications securely, out of sight and out of reach.
- Reviewing the dosing schedule and maintaining a routine for tracking symptoms.
- Staying in regular communication with healthcare providers about any concerns.
A well-organized supervision plan helps maintain safety from the start of treatment through its completion.
Overdosage
Signs and symptoms of chloroquine toxicity
A large overdose of chloroquine can escalate rapidly, becoming life-threatening within a short period.
Early detection of toxicity is especially important in children and smaller adults, who are particularly at risk.
Typical manifestations often span multiple organ systems, such as:
- Cardiovascular instability, including abnormal blood pressure, extremely slow or rapid heart rates, conduction disturbances, and dangerous arrhythmias.
- Severe central nervous system involvement—agitation, confusion, seizures, loss of consciousness, and ultimately coma.
- Respiratory compromise is marked by reduced breathing effort, inadequate ventilation, or episodes of sleep apnea.
- Metabolic derangements such as significant hypokalemia, acid–base imbalance, and possible hypoglycemia.
- Gastrointestinal symptoms like nausea, vomiting, and abdominal discomfort sometimes serve as early indicators of systemic toxicity.
These symptoms can intensify abruptly, leaving only a narrow window for timely intervention.
Emergency response and initial management
Any suspected chloroquine overdose should be treated as a medical emergency.
Immediate professional help is essential; trying to handle the situation at home is unsafe and inadequate.
In a clinical setting, the first priorities typically include:
- Assessing airway, breathing, and circulation, followed by rapid stabilization of vital functions.
- Continuous monitoring of cardiac activity and hemodynamic status to detect arrhythmias early and prevent collapse.
- Prompt supportive care focused on improving oxygenation, maintaining blood pressure, and correcting metabolic abnormalities.
- If the patient arrives quickly and the airway is protected, clinicians may consider activated charcoal as part of decontamination.
Because the drug carries a high risk of rapid, severe deterioration, urgent transfer to a facility capable of intensive monitoring is strongly recommended.
Long-term complications from overdose
Individuals who recover from a chloroquine overdose may continue to face after-effects that appear later or persist over time.
Often, these longer-term problems only become evident once the initial crisis has passed.
Potential late-emerging complications include:
- Eye damage—ongoing visual disturbances, scotomas, or structural retinal changes that remain after exposure.
- Cardiac issues—persistent conduction abnormalities or evolving problems in those who had significant heart involvement.
- Neurological problems—cognitive changes, neuropathy, or lasting motor weakness, often linked to periods of low oxygen or seizure activity.
- Psychological impacts—such as anxiety, post-event stress reactions, or depression related to the experience.
Long-term follow-up with appropriate specialists is important for identifying and managing these delayed complications.
Handling Precautions
Safe storage and handling of suspension
Suspension formulations must be handled with care to maintain their stability and prevent accidental ingestion.
A few simple steps can significantly reduce both degradation and the risk of misuse.
Key recommendations include:
- Store the medication out of children’s sight and reach—preferably in a locked cabinet or on a high shelf.
- Keep the bottle tightly closed to prevent contamination, spills, and loss of volatile components.
- Shake the bottle before each dose to ensure the active ingredient is evenly dispersed.
- Avoid transferring the suspension to another container, as this increases the likelihood of confusion and dosing mistakes.
Using a careful, structured approach helps preserve safety and maintain the product’s integrity.
Measuring and administration accuracy
Accurate measurement of a suspension is essential, as the margin between a correct dose and an excessive one is extremely narrow.
Even a slight volume error can alter the amount of medication actually given.
To keep dosing precise:
- Use a calibrated syringe, dosing cup, or pharmacist-provided measuring spoon.
- Avoid household teaspoons or tablespoons, which vary widely in volume and are unreliable.
- Check the calibration marks and align the liquid’s meniscus with the intended measurement line.
- Administer the dose immediately after measuring to prevent the suspension from settling and changing concentration.
When dosing technique is consistent, fluctuations in drug exposure are minimized, making treatment outcomes more predictable.
Disposal considerations
Expired or unused suspension should never be thrown out casually.
Improper disposal can create avoidable safety risks and environmental harm.
Preferred disposal methods include:
- Using local pharmacy take-back programs, which ensure medications are destroyed safely.
- Avoiding disposal in household sinks or toilets unless local regulations specifically allow it, as this helps prevent contamination.
- If no other option is available, render the product unusable before placing it in the trash—for example, by mixing it with coffee grounds or used cat litter and sealing it in a container.
Responsible disposal does more than clean up; it helps protect children, pets, and the surrounding environment.

Storage
Recommended temperature conditions
Maintaining proper temperature is essential for preserving a suspension’s stability and effectiveness.
Most formulations should be kept at controlled room temperature unless the label specifies otherwise.
Key storage recommendations include:
- Keep the product at about 20 °C to 25 °C unless different instructions are provided.
- Avoid exposing the bottle to extreme heat or cold, as temperature swings can change viscosity, cause crystallization, or affect drug solubility.
- Do not store the suspension in a car or near heat sources, where temperatures can fluctuate widely.
Keeping the product within its recommended temperature range helps maintain its reliability over time.
Protection from light and moisture
Light and moisture can trigger degradation of both the active ingredient and the excipients.
Even a small, noticeable change in the suspension’s appearance may signal a deeper loss of stability.
To protect the product, the following practices are recommended:
- Keep the suspension in its original container, as these bottles are designed to block light exposure.
- Make sure the cap is tightly closed after every use to prevent moisture intrusion.
- Avoid storing the medication in bathrooms or other humid areas, which are prone to condensation and temperature fluctuations.
- A dry, shaded storage environment helps maintain the suspension’s quality over time.
Shelf-life and expiration guidelines
Every suspension has a defined shelf life, and once that period ends, its safety and effectiveness can no longer be guaranteed.
Both the manufacturer’s printed expiration date and any beyond-use date assigned after opening must be followed.
Key points include:
- Check the labeled expiration date before starting each treatment course.
- Follow any “use within X days after opening” instructions, as many suspensions degrade quickly once exposed to air or frequent handling.
- Discard the product if it shows any changes—such as altered color, odor, or clumping—even if it has not yet reached its expiration date.
Adhering to these shelf-life and expiration guidelines helps ensure that the medication remains potent and safe for patient use.
Nivaquine P Suspension, Chloroquine FAQ
- Can Chloroquine cause diarrhea?
- Does Chloroquine cause itching?
- What to avoid when taking Chloroquine?
- Why is it becoming more difficult to treat malaria using Chloroquine?
- What are the three uses of Chloroquine?
- Is Chloroquine safe in breastfeeding?
- What are the side effects of Chloroquine?
- What is the drug Chloroquine used for?
- What are the main uses of Chloroquine in medicine?
- Which pharmacies offer Chloroquine with home delivery?
- What are the side effects of Chloroquine I should be aware of?
- How does Chloroquine compare to other antimalarial drugs in effectiveness?
- What are the side effects of Chloroquine I should be aware of?
- Is Chloroquine safe to use for autoimmune diseases?
- Can Chloroquine injection be given iv?
- Can Chloroquine cause miscarriage?
- Can Chloroquine cure malaria?
- Can Chloroquine be given in pregnancy?
- Can Chloroquine cure typhoid?
- Can Chloroquine injection cause miscarriage?
- Can Chloroquine cause itching?
- Can Chloroquine injection be given to a pregnant woman?
- Can Chloroquine affect pregnancy?
- Can Chloroquine cause hiccups?
- Can Chloroquine treat typhoid?
- Can Chloroquine be taken with paracetamol?
- Can I buy Chloroquine over the counter?
- How Chloroquine works?
- How Chloroquine works in malaria?
- How Chloroquine works in rheumatoid arthritis?
- How Chloroquine is made?
- How does Chloroquine treat malaria?
- How does Chloroquine prevent malaria?
- How Chloroquine is useful as an antimalarial?
- What is Chloroquine phosphate?
- What does Chloroquine treat?
- What does Chloroquine do to the body?
- When was Chloroquine discovered?
- Who should not take Chloroquine?
- Is Chloroquine an anti-inflammatory?
- How long does Chloroquine last in the body?
- What is the toxic effect of Chloroquine?
- Does Chloroquine affect the heart?
- Does Chloroquine cause weight gain?
- Does Chloroquine lower blood pressure?
- What to avoid when taking Chloroquine?
- Can Chloroquine cause fatigue?
- What are the psychiatric side effects of Chloroquine?
- Does Chloroquine cause vision problems?
- How does Chloroquine affect the skin?
- What are the psychiatric side effects of Chloroquine?
- Does Chloroquine cause vision problems?
- How to stop Chloroquine reaction?
- Are there alternatives to Chloroquine?
- Does Chloroquine affect blood pressure?
- Where is Chloroquine found naturally?
Can Chloroquine cause diarrhea?
Chloroquine can sometimes cause diarrhea in people because it irritates the gastrointestinal tract.
Does Chloroquine cause itching?
Chloroquine can cause an itching sensation in people with deeper complexions and the itch can, at times, be fairly intense.
What to avoid when taking Chloroquine?
During chloroquine therapy, it’s prudent to avoid alcohol and only take antacids several hours apart from the dose, and steer clear of any other drugs that might lengthen the heart’s rhythm unless a clinician has given clearance.
Why is it becoming more difficult to treat malaria using Chloroquine?
The difficulty of malaria treatment has increased because parasites, especially Plasmodium falciparum, have developed widespread resistance to Chloroquine.
What are the three uses of Chloroquine?
Chloroquine serves three main purposes: preventing malaria, treating malaria in areas where parasites are sensitive to it, and managing specific autoimmune diseases like rheumatoid arthritis.
Is Chloroquine safe in breastfeeding?
Chloroquine is generally safe while breastfeeding because the amount the infant receives through milk is usually low, though a doctor should still confirm the appropriate dosage.
What are the side effects of Chloroquine?
Some individuals experience dizziness from Chloroquine, often because the drug affects their inner ear or how their blood pressure is regulated.
What is the drug Chloroquine used for?
The main uses of Chloroquine are to prevent and treat malaria where the parasites are still susceptible, and to manage specific inflammatory and autoimmune diseases.
What are the main uses of Chloroquine in medicine?
Chloroquine's primary medical applications are treating and preventing malaria, along with the long-term management of certain autoimmune conditions like lupus and rheumatoid arthritis.
Which pharmacies offer Chloroquine with home delivery?
While many licensed online and local pharmacies offer home delivery of Chloroquine, availability and the requirement for a valid prescription depend on the country.
What are the side effects of Chloroquine I should be aware of?
Common side effects of Chloroquine include nausea, headache, stomach upset, dizziness, blurred vision, and itching; however, rare but serious complications, like heart rhythm problems or retinal damage, can occur with extended use.
How does Chloroquine compare to other antimalarial drugs in effectiveness?
Chloroquine is only effective in areas where malaria parasites have not developed resistance; in contrast, newer drugs like artemisinin-based combinations are much more dependable in regions dominated by resistant strains.
What are the side effects of Chloroquine I should be aware of?
Side effects of Chloroquine include digestive issues, changes in vision, mood alteration, and itching; high or prolonged doses may also potentially harm the retina or heart rhythm.
Is Chloroquine safe to use for autoimmune diseases?
When Chloroquine is used for autoimmune conditions, safety depends on proper monitoring, including regular eye exams and adjusting the dosage based on the patient's weight and risk factors.
Can Chloroquine injection be given iv?
Because of the high risk of severe cardiac toxicity, Chloroquine should not generally be injected intravenously; instead, it is typically administered intramuscularly when required.
Can Chloroquine cause miscarriage?
Standard preventive or treatment doses of Chloroquine are not known to cause miscarriage, though toxic or misused doses can be harmful to both the mother and the fetus.
Can Chloroquine cure malaria?
Chloroquine effectively cures malaria caused by sensitive strains, particularly Plasmodium vivax and Plasmodium ovale, but it cannot treat infections caused by resistant Plasmodium falciparum.
Can Chloroquine be given in pregnancy?
Standard doses of Chloroquine used for preventing or treating malaria are generally considered safe during pregnancy, supported by its extensive clinical history in this context.
Can Chloroquine cure typhoid?
Chloroquine cannot cure typhoid; since typhoid is a bacterial infection, it requires specific antibiotics, not antimalarial treatment.
Can Chloroquine injection cause miscarriage?
When Chloroquine injection is used at the correct therapeutic dose, it is not known to cause miscarriage, although maternal risks exist with overdosing or improper administration.
Can Chloroquine cause itching?
Itching is a common side effect of Chloroquine, which may be more severe in specific populations due to heightened genetic or skin sensitivity.
Can Chloroquine injection be given to a pregnant woman?
While Chloroquine injection may be used in pregnancy when clearly necessary, as standard doses are usually safe, its application requires careful assessment and monitoring by a doctor.
Can Chloroquine affect pregnancy?
Routine preventive or treatment doses of Chloroquine are generally safe for pregnancy, but excessive or incorrect use can pose risks to the mother and the fetus.
Can Chloroquine cause hiccups?
Hiccups are not a typical side effect of Chloroquine, but they can occasionally result from the gastrointestinal irritation or reflux that the drug sometimes causes.
Can Chloroquine treat typhoid?
Typhoid cannot be treated with Chloroquine because it is a bacterial infection that requires antibiotics, not antimalarial drugs.
Can Chloroquine be taken with paracetamol?
Taking Chloroquine with Paracetamol is generally acceptable, as these two medications do not have significant interactions at typical doses.
Can I buy Chloroquine over the counter?
Chloroquine usually requires a prescription and is not sold over the counter because of the necessary safety monitoring, careful dosing, and concerns about drug resistance.
How Chloroquine works?
How Chloroquine works in malaria?
When treating malaria, Chloroquine accumulates in the parasite's food vacuole, which prevents the parasite from detoxifying heme and consequently kills it.
How Chloroquine works in rheumatoid arthritis?
In the treatment of rheumatoid arthritis, Chloroquine decreases excessive immune response by regulating lysosomal activity and reducing inflammatory processes.
How Chloroquine is made?
Chloroquine is created in a lab by combining specific aromatic compounds and amine groups through a multi-step chemical synthesis process under precise control.
How does Chloroquine treat malaria?
Chloroquine treats malaria by stopping the parasite from neutralizing toxic heme, which leads to the parasite's death inside the red blood cells.
How does Chloroquine prevent malaria?
Chloroquine prevents malaria by keeping enough of the drug in the bloodstream to stop the early replication of the parasite before the infection can become serious.
How Chloroquine is useful as an antimalarial?
Chloroquine is effective against malaria because it gathers in infected cells and quickly interrupts the parasite's vital metabolic functions.
What is Chloroquine phosphate?
Chloroquine Phosphate is the stable salt form of chloroquine used in injections and tablets to enhance the drug's absorption.
What does Chloroquine treat?
Chloroquine is used to treat malaria caused by susceptible strains and to help manage autoimmune conditions like lupus and rheumatoid arthritis.
What does Chloroquine do to the body?
Chloroquine works by building up inside cells, changing parasite metabolism, and adjusting immune activity, but its dosage and duration of use can also affect the eyes, heart, and digestive system.
When was Chloroquine discovered?
Chloroquine was first created in the 1930s and became a significant antimalarial drug when it was introduced for clinical use in the 1940s.
Who should not take Chloroquine?
Chloroquine should generally be avoided by individuals with pre-existing conditions such as retinal disease, certain heart rhythm issues, severe liver problems, epilepsy, or known Chloroquine hypersensitivity, unless a specialist advises its use.
Is Chloroquine an anti-inflammatory?
Because Chloroquine has anti-inflammatory and immune-modulating properties, it is prescribed for autoimmune diseases like lupus and rheumatoid arthritis.
How long does Chloroquine last in the body?
Chloroquine stays in the body for a long time—often weeks—due to its long half-life, with its storage in tissues extending its activity.
What is the toxic effect of Chloroquine?
High or repeated excessive doses of Chloroquine can cause toxicity, which may result in dangerous heart rhythm disturbances, severe hypotension, seizures, respiratory failure, and retinal damage.
Does Chloroquine affect the heart?
Chloroquine can impact the heart by extending electrical conduction time, potentially causing irregular heart rhythms (arrhythmias), particularly in cases of overdose or when taken with other similar-risk drugs.
Does Chloroquine cause weight gain?
Chloroquine is not typically linked to weight gain and generally does not significantly affect a person's body weight.
Does Chloroquine lower blood pressure?
Chloroquine does not usually reduce blood pressure, although high doses can rarely cause blood pressure to fluctuate.
What to avoid when taking Chloroquine?
When on Chloroquine, you should avoid excessive alcohol intake, taking antacids near your dose time, and using any other medication that significantly affects your heart rhythm unless explicitly approved by your doctor.
Can Chloroquine cause fatigue?
Some people experience fatigue while taking Chloroquine, which is often linked to its effects on sleep, mood, or their general tolerance for the drug.
What are the psychiatric side effects of Chloroquine?
Fatigue is a possible side effect of Chloroquine, often stemming from its impact on sleep, mood, or the individual's overall tolerance to the medicine.
Does Chloroquine cause vision problems?
Chloroquine may cause blurred vision or difficulty focusing, and long-term use can potentially harm the retina, highlighting the necessity of regular eye exams.
How does Chloroquine affect the skin?
Skin reactions to Chloroquine can range from mild to persistent and include itching, rashes, skin darkening, or greater sensitivity to sunlight.
What are the psychiatric side effects of Chloroquine?
In susceptible individuals, especially with extended use, Chloroquine may occasionally cause agitation, difficulty sleeping, mood changes, or more severe mental health symptoms.
Does Chloroquine cause vision problems?
Chloroquine can affect near vision or cause halos around lights, and if chronic use is not monitored, there is a small but significant risk of retinal damage.
How to stop Chloroquine reaction?
Managing a Chloroquine reaction usually involves discontinuing the drug under a doctor's supervision, treating any symptoms like itching or rash, and substituting it with a safer medication if necessary.
Are there alternatives to Chloroquine?
Depending on the medical requirement, alternatives to Chloroquine include artemisinin-based drugs for malaria, or Hydroxychloroquine and other immune-modulating drugs for autoimmune diseases.
Does Chloroquine affect blood pressure?
Chloroquine typically has no effect on blood pressure, though mild fluctuations—either increases or decreases—have rarely been reported, especially when high doses or injections are administered.
Where is Chloroquine found naturally?
Chloroquine is entirely synthetic and does not exist in nature, although its creation was historically inspired by quinine, a compound extracted from cinchona bark.
Popular Products





Similar Product

