Sematrinity Pen Injection, Semaglutide
- 1. Introduction to Sematrinity Pen Injection (Semaglutide)
- 2. Composition and Formulation Details
- 3. Mechanism of Action: How Sematrinity Works
- 4. Approved Medical Uses of Sematrinity Pen Injection
- 5. Off-Label Uses and Emerging Clinical Applications
- 6. Dosage and Administration Guidelines
- 7. Side Effects of Sematrinity Pen Injection
- 8. Serious and Rare Adverse Reactions
- 9. Drug Interactions and Concomitant Use
- 10. Contraindications
- 11. Warnings and Safety Considerations
- 12. Careful Administration and Clinical Monitoring
- 13. Important Precautions Before and During Use
- 14. Administration in Special Populations
- 14.1 Administration to Elderly Patients
- 14.1.1 Dose Considerations and Comorbidity Management
- 14.1.2 Increased Sensitivity to Adverse Effects
- 14.2 Administration to Pregnant Women and Nursing Mothers
- 14.2.1 Risk-Benefit Assessment in Pregnancy
- 14.2.2 Potential Effects on Fetal Development
- 14.2.3 Excretion in Breast Milk and Recommendations
- 14.3 Administration to Pediatric Patients
- 14.3.1 Safety and Efficacy in Children and Adolescents
- 14.3.2 Age Restrictions and Clinical Guidelines
- 15. Overdosage and Emergency Management
- 16. Storage and Stability Requirements
- 17. Handling and Injection Precautions
- 18. Patient Counseling and Practical Tips
1. Introduction to Sematrinity Pen Injection (Semaglutide)
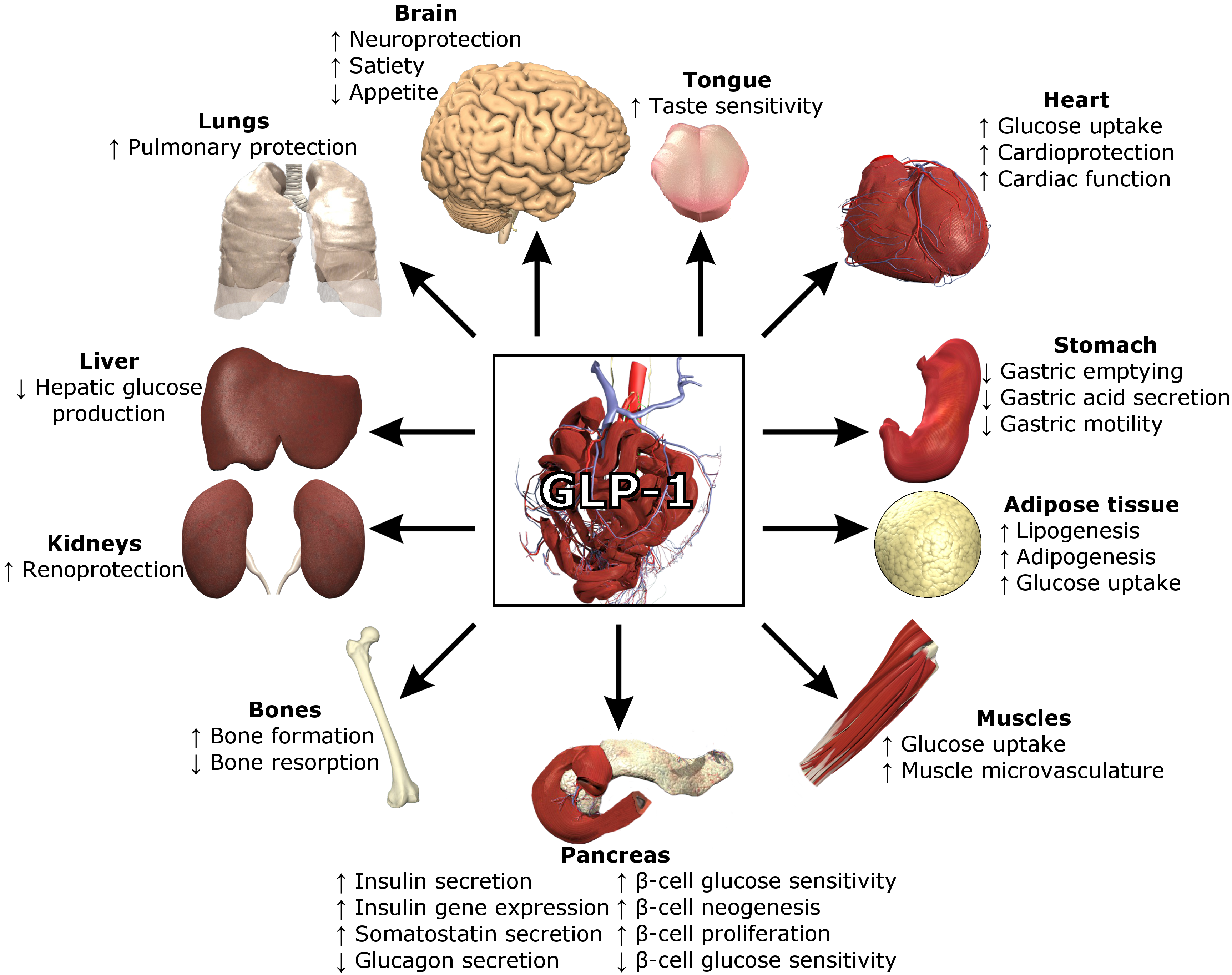
1.1 Overview of Semaglutide as a GLP-1 Receptor Agonist
Semaglutide is a synthetic analogue of the endogenous incretin hormone GLP-1 (glucagon-like peptide-1). It exerts profound metabolic effects by enhancing glucose-dependent insulin secretion while attenuating glucagon output. This duality confers both glycemic stability and reduced risk of hypoglycemia when used appropriately.
- Enhances insulin release in hyperglycemic states
- Suppresses hepatic glucose production
- Promotes satiety and weight reduction
1.2 Brand Profile: What is Sematrinity Pen Injection?
Sematrinity Pen Injection is a prefilled, user-friendly delivery system containing semaglutide for subcutaneous administration. Designed for weekly dosing, it provides sustained pharmacological activity with minimal dosing burden. Its ergonomic configuration facilitates precise dosing and adherence.

1.3 Therapeutic Class and Clinical Significance
This medication belongs to the incretin mimetic class, specifically GLP-1 receptor agonists. It represents a paradigm shift in metabolic therapeutics, addressing both hyperglycemia and excess adiposity with a single molecular intervention.
1.4 Indications Approved by Regulatory Authorities
Sematrinity is primarily indicated for:
- Type 2 diabetes mellitus management
- Adjunct therapy to diet and exercise
- Reduction of cardiovascular risk in select populations
1.5 Growing Role in Metabolic Disease Management
With the escalating prevalence of metabolic syndrome, semaglutide-based therapies have become integral. They address not only glycemic dysregulation but also obesity and cardiometabolic risk, thereby redefining comprehensive disease management.
2. Composition and Formulation Details
2.1 Active Ingredient: Semaglutide:Structure and Properties
Semaglutide is a long-acting peptide engineered for enhanced stability against enzymatic degradation. Its structural modifications allow prolonged receptor engagement and once-weekly dosing.
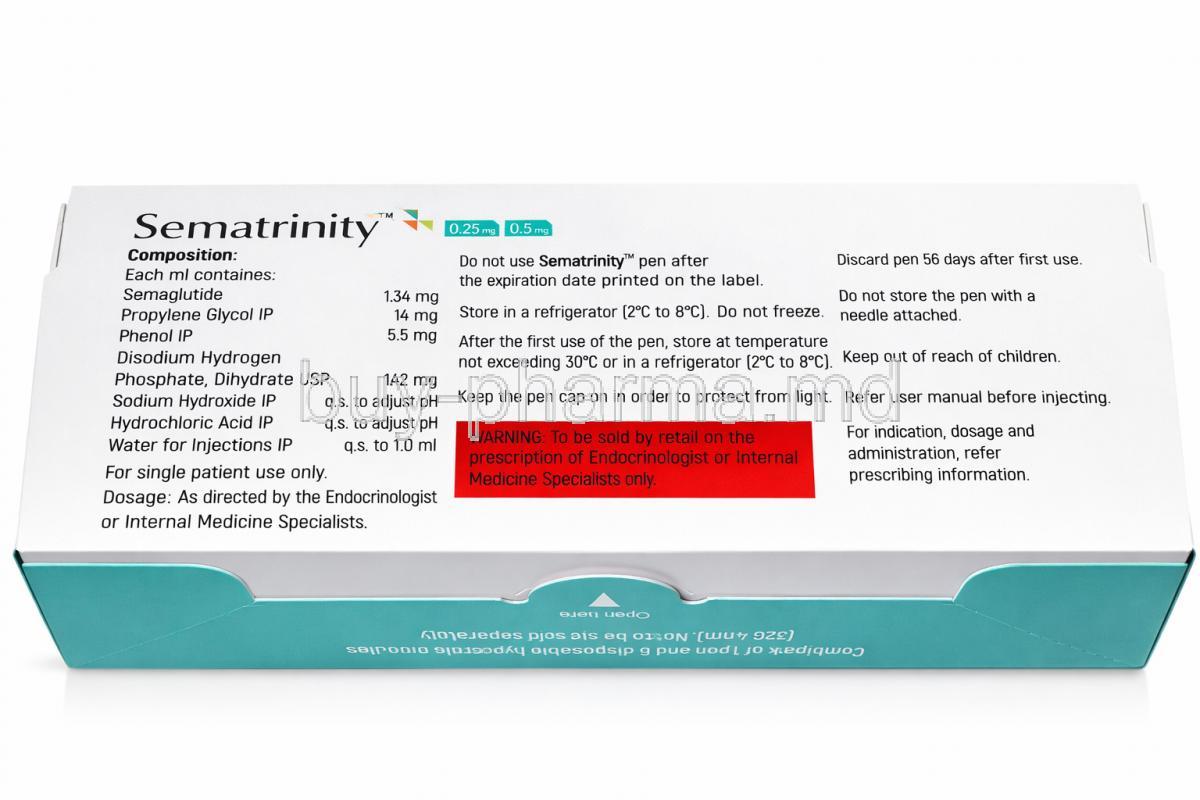
2.2 Excipients and Inactive Components in the Pen
The formulation includes stabilizers, buffers, and isotonic agents that ensure physicochemical stability. These excipients preserve the integrity of the peptide during storage and administration.
2.3 Prefilled Pen Design and Delivery Mechanism
The pen utilizes a precision dosing mechanism, delivering consistent volumes with minimal user error. Its design reduces variability and improves patient compliance.
2.4 Available Strengths and Dosage Variants
Common strengths include:
- 0.25 mg (initiation dose)
- 0.5 mg (maintenance dose)
- 1 mg or higher (advanced glycemic control)
2.5 Pharmacokinetic Profile
Semaglutide exhibits a prolonged half-life of approximately one week. It demonstrates slow absorption, extensive plasma protein binding, and minimal renal excretion of intact drug.
Sublingual semaglutide
Sublingual semaglutide is a type of medicine you take by placing drops under your tongue. It's used to help people with type 2 diabetes and to lose weight. This medicine is different because it doesn't need a needle, and it gets absorbed into your bloodstream right through your mouth. That means it bypasses your digestive system, which helps your body absorb it more effectively. It's a good alternative for people who don't like getting injections.
Compounded semaglutide with b12
Compounded semaglutide with B12 combines a GLP-1 receptor agonist for weight loss and blood sugar control with Vitamin B12, often added to support energy metabolism and potentially reduce side effects.
Liraglutide vs semaglutide
Semaglutide is generally more effective for weight loss and blood sugar management than liraglutide (Saxenda/Victoza). Semaglutide is injected weekly, offering greater results, roughly 15% body weight loss, compared to daily injections of liraglutide, which typically yield 6-8% weight loss. Both are GLP-1 receptor agonists with similar gastrointestinal side effects.
Metformin vs semaglutide
Metformin reduces hepatic glucose production. Semaglutide mimics the GLP-1 hormone to increase insulin secretion, slow stomach emptying, and reduce appetite. Semaglutide results in significantly more weight loss, often making it preferred for obesity.
Difference between semaglutide and tirzepatide
Tirzepatide and Semaglutide (Ozempic/Wegovy) are highly effective weekly injections for diabetes and weight loss, but they differ in mechanism and potency. Tirzepatide is a dual agonist (GIP and GLP-1), which clinical trials indicate causes greater weight loss (up to 20-21%) than the GLP-1-only agonist Semaglutide (around 15%), though both are effective tools for managing obesity.
3. Mechanism of Action: How Sematrinity Works
3.1 GLP-1 Receptor Activation and Insulin Secretion Enhancement
Upon receptor activation, semaglutide amplifies insulin secretion in a glucose-dependent manner. This ensures efficacy without excessive hypoglycemia.
3.2 Suppression of Glucagon Release
It inhibits glucagon secretion, thereby reducing hepatic gluconeogenesis. The result is improved fasting and postprandial glucose levels.
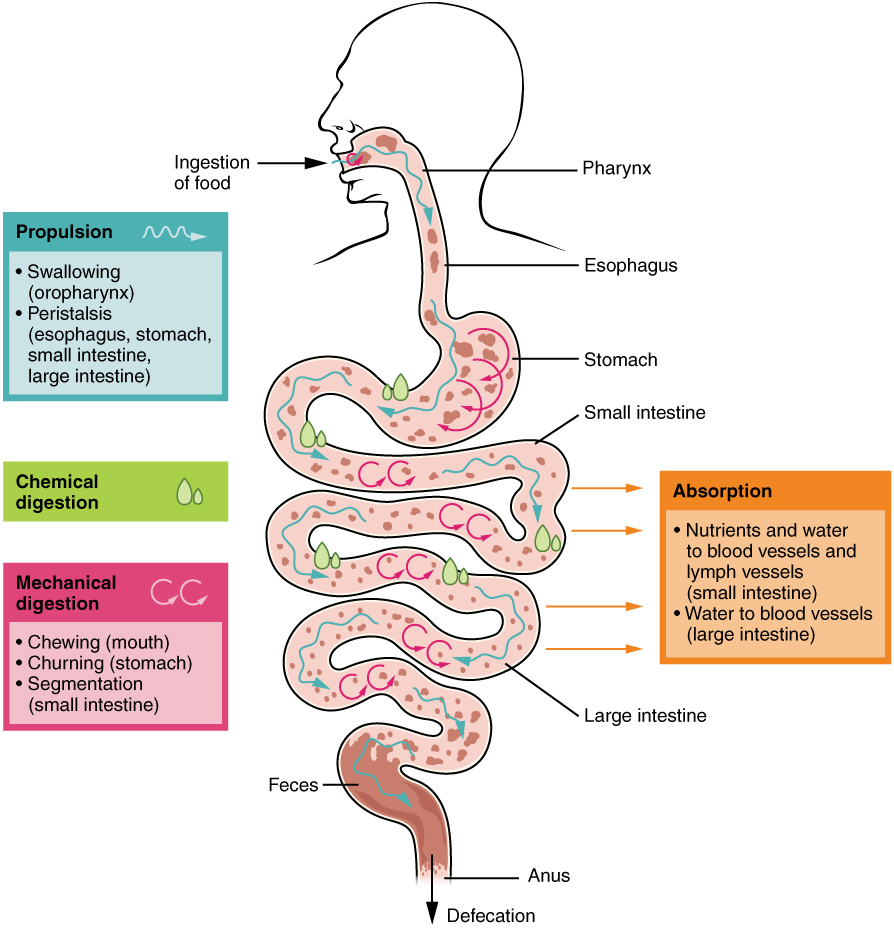
3.3 Delayed Gastric Emptying and Appetite Regulation
Gastric motility is decelerated. Nutrient absorption is prolonged, leading to reduced postprandial glucose spikes and enhanced satiety.
3.4 Central Nervous System Effects on Satiety
Semaglutide acts on hypothalamic centers, modulating appetite signals. This neuroendocrine effect contributes to sustained weight loss.
3.5 Impact on Cardiovascular Risk Factors
It improves lipid profiles, reduces body weight, and lowers blood pressure. These cumulative effects diminish cardiovascular morbidity.
4. Approved Medical Uses of Sematrinity Pen Injection
4.1 Management of Type 2 Diabetes Mellitus
4.2 Glycemic Control in Combination Therapy
It may be combined with:
4.3 Reduction of Cardiovascular Risk

4.4 Role in Long-Term Diabetes Management Plans
Its once-weekly regimen enhances adherence. Long-term use supports durable glycemic control and weight management.
5. Off-Label Uses and Emerging Clinical Applications
5.1 Weight Loss and Obesity Management

5.2 Semaglutide for PCOS
5.3 Non-Alcoholic Fatty Liver Disease (NAFLD/NASH)
Emerging data suggest a reduction in hepatic steatosis and inflammation.
5.4 Prediabetes and Metabolic Syndrome
Early intervention with semaglutide may delay progression to overt diabetes.
5.5 Appetite Control in Binge Eating Disorders
By modulating satiety pathways, it may reduce compulsive eating behaviors.

5.6 Cardiometabolic Optimization
Its pleiotropic effects extend beyond glucose lowering, improving overall metabolic health.
6. Dosage and Administration Guidelines
6.1 Initial Dosing and Titration Schedule
Treatment typically begins at a low dose to enhance tolerability. Gradual titration minimizes gastrointestinal discomfort.
Semaglutide weight loss dosage chart
- Weeks 1-4: 0.25 mg, weekly injection dosage
- Weeks 4-8: 0.5 mg, weekly injection dosage
- Weeks 8-12: 1 mg, weekly injection dosage
- Weeks 13+: Up to 2.4 mg, weekly injection dosage
Semaglutide dosage in units
- 10-15 units each week for the first 4 weeks
- 15-20 units each week for 2 weeks
- 20-25 units each week for 3 weeks
- 30-50 units each week weeks 10 and onward
Microdose semaglutide
When it comes to taking semaglutide, some people start with a really small dose and gradually increase it over time - this is called microdosing. This approach can be especially helpful for certain patients, like those who are highly sensitive to medications and might get nausea or other side effects easily. It's also good for first-time users who need a little extra time to get used to the treatment. And for patients with a lower body mass index, or BMI, microdosing can be a better option because they might not need as high of a dose. By starting small and increasing the dose slowly, these patients can benefit from the medication while minimizing risks. This way, they can adjust to the treatment at their own pace and reduce the likelihood of unpleasant side effects.
6.2 Weekly Injection Protocol and Timing
The injection is administered once weekly, regardless of meals. Consistency in timing is recommended.
6.3 Semaglutide injection sites
- Abdomen
- Thigh
- Upper arm
Rotation of sites prevents localized irritation.

6.4 Dose Escalation to Minimize Gastrointestinal Effects
Incremental increases allow physiological adaptation, reducing nausea and vomiting.
6.5 Missed Dose Management
If a dose is missed, it should be administered promptly within a defined window. Otherwise, resume the next scheduled dose.
6.6 Switching from Other GLP-1 Receptor Agonists
Transition requires clinical judgment. Overlapping therapy should be avoided.
Switching from semaglutide to tirzepatide
When you switch from semaglutide to tirzepatide, known as Mounjaro or Zepbound, you usually need to wait for a week after your last injection. Then you start with a low dose, either 2.5mg or 5mg, to try to minimize any side effects. This change can be really helpful if you've stopped losing weight, because tirzepatide works in two ways, with GIP and GLP-1, which might make it more effective.
7. Side Effects of Sematrinity Pen Injection
7.1 Common Side Effects

7.2 Gastrointestinal Tolerability
Symptoms often diminish with continued use. Dose titration plays a crucial role in mitigation.
7.3 Injection Site Reactions
Mild erythema or discomfort may occur at the injection site.
7.4 Fatigue, Headache, and Dizziness
These nonspecific symptoms may arise during initial therapy phases.

7.5 Appetite Suppression and Weight Changes
Reduced caloric intake contributes to gradual and sustained weight loss.
7.6 Semaglutide hair loss
Losing weight with Semaglutide can sometimes lead to temporary hair loss, called telogen effluvium. This usually happens because of rapid weight loss, not having enough essential nutrients like iron, zinc, and protein, or hormonal changes. It's worth noting that not many people experience this side effect, and it often goes away on its own within 3 to 6 months once your weight becomes more stable.

8. Serious and Rare Adverse Reactions
8.1 Risk of Pancreatitis
Severe abdominal pain may indicate pancreatitis and requires immediate evaluation.
8.2 Thyroid C-Cell Tumor Risk
Preclinical studies suggest a potential risk. Clinical relevance remains under surveillance.
8.3 Hypoglycemia
Risk increases when combined with insulin or sulfonylureas.
8.4 Gallbladder Disease
Rapid weight loss may predispose to cholelithiasis.
8.5 Renal Impairment
Dehydration secondary to gastrointestinal effects may compromise renal function.
8.6 Hypersensitivity Reactions
Rare but potentially severe allergic responses may occur.
Tirzepatide vs. Semaglutide Side Effects
When people first start taking these two drugs, they often feel sick to their stomach. This can lead to nausea, vomiting, and diarrhea, or sometimes the opposite - constipation and abdominal pain. It's like their body is trying to get used to the new medicine. Some research shows that both drugs work well, but a little more people might be able to stick with tirzepatide than with a high dose of semaglutide, because they don't get as sick from the side effects.
9. Drug Interactions and Concomitant Use
9.1 Interaction with Insulin and Oral Agents
Concurrent use may necessitate dose adjustments to prevent hypoglycemia.
9.2 Delayed Gastric Emptying Effects
Absorption of oral medications may be altered, particularly those with narrow therapeutic indices.
9.3 Interaction with Anticoagulants
Monitoring is advised when used with warfarin due to potential variability in absorption.
9.4 Use with Weight Loss Medications
Combination therapy should be approached cautiously due to additive effects.
9.5 Alcohol Interaction
Alcohol may exacerbate glycemic fluctuations and gastrointestinal symptoms.
10. Contraindications
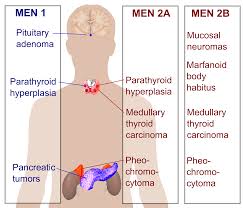
10.1 History of Medullary Thyroid Carcinoma
Use is contraindicated in individuals with personal or familial history of MTC.
10.2 Multiple Endocrine Neoplasia Syndrome Type 2
Patients with MEN2 should avoid semaglutide therapy.
10.3 Hypersensitivity to Semaglutide
Known allergic reactions preclude its use.
10.4 Severe Gastrointestinal Disorders
Conditions such as gastroparesis may be exacerbated.
10.5 Pregnancy Considerations
Use during pregnancy is generally not recommended unless clearly necessary.

11. Warnings and Safety Considerations
11.1 Risk of Thyroid Tumors and Monitoring Recommendations
Semaglutide has been associated with thyroid C-cell tumors in preclinical studies. Although the direct clinical relevance in humans remains under evaluation, vigilance is imperative. Patients should be informed about potential symptoms such as neck swelling, dysphagia, or persistent hoarseness.
- Routine monitoring of thyroid function may be considered
- Avoid use in patients with a history of medullary thyroid carcinoma
- Evaluate unexplained thyroid nodules promptly

11.2 Pancreatitis Risk and Clinical Vigilance
Acute pancreatitis, though infrequent, represents a serious adverse event. Clinicians should maintain a high index of suspicion when patients report severe abdominal pain radiating to the back.
Immediate discontinuation is warranted if pancreatitis is suspected. Rechallenge is generally discouraged.
11.3 Hypoglycemia Risk with Combination Therapy
While semaglutide alone carries a low intrinsic risk of hypoglycemia, concomitant use with insulin or sulfonylureas may potentiate this effect. Dose adjustments of co-administered agents are often necessary.
- Monitor blood glucose levels closely
- Educate patients on recognizing hypoglycemic symptoms
- Adjust therapy based on glycemic response
11.4 Dehydration and Electrolyte Imbalance
Gastrointestinal adverse effects such as vomiting and diarrhea may lead to fluid depletion. This can precipitate electrolyte disturbances and renal compromise.
Maintaining hydration is essential. Patients should be advised to increase fluid intake, particularly during periods of gastrointestinal distress.
11.5 Vision Changes and Diabetic Retinopathy Complications
Rapid improvement in glycemic control may transiently worsen diabetic retinopathy. Visual disturbances should be evaluated without delay.
- Regular ophthalmologic assessments are recommended
- Monitor patients with pre-existing retinopathy closely
11.6 Not losing weight on semaglutide
It's not uncommon for people to struggle with weight loss when they first start taking semaglutide. This can happen for a few reasons. Sometimes the dose is too low, and it takes a few months to reach the right amount. It can take around 3 to 4 months to reach the full dose that actually works. There are a few key things that can get in the way of weight loss. Eating a poor diet, not getting enough exercise, and having issues with your metabolism, sleep, or stress levels can all make it harder to lose weight.
12. Careful Administration and Clinical Monitoring
12.1 Use in Patients with Renal Impairment
Although semaglutide is not primarily renally excreted, dehydration secondary to gastrointestinal symptoms may exacerbate renal dysfunction. Caution is advised in patients with compromised renal reserve.
12.2 Use in Hepatic Dysfunction
Hepatic impairment does not significantly alter semaglutide pharmacokinetics. However, clinical prudence is warranted due to potential metabolic variability.
12.3 Monitoring Blood Glucose and HbA1c Levels
Regular monitoring of glycemic indices is fundamental to therapeutic success. HbA1c provides a longitudinal assessment, while self-monitoring of blood glucose offers immediate feedback.
- Assess HbA1c every 3-6 months
- Adjust therapy based on trends and targets
12.4 Monitoring Body Weight and Nutritional Status
Weight reduction is a therapeutic goal but must be balanced against nutritional adequacy. Excessive weight loss may indicate intolerance or overmedication.
12.5 Dose Adjustments in Sensitive Populations
Patients with multiple comorbidities or heightened sensitivity may require individualized dosing strategies. Gradual titration is essential in such cohorts.
13. Important Precautions Before and During Use
13.1 Gradual Dose Escalation to Improve Tolerability
Initiating therapy at a low dose and escalating incrementally allows physiological adaptation. This mitigates gastrointestinal discomfort and enhances adherence.
13.2 Avoiding Abrupt Discontinuation
Sudden cessation may lead to rebound hyperglycemia. A structured discontinuation plan is preferable when therapy needs to be halted.
13.3 Maintaining Adequate Hydration
Hydration plays a pivotal role in preventing renal complications and maintaining electrolyte equilibrium. This is particularly important during episodes of nausea or vomiting.
13.4 Recognizing Early Signs of Adverse Effects
Early identification of adverse reactions facilitates timely intervention. Patients should be counseled to report unusual symptoms promptly.
13.5 Adherence to Weekly Dosing Schedule
Consistency is critical. Administering the injection on the same day each week ensures stable plasma concentrations and optimal efficacy.
14. Administration in Special Populations
14.1 Administration to Elderly Patients
14.1.1 Dose Considerations and Comorbidity Management
Elderly patients often present with polypharmacy and multiple comorbidities. Dose adjustments may be required to minimize adverse outcomes.
14.1.2 Increased Sensitivity to Adverse Effects
Age-related physiological changes may amplify drug effects. Close monitoring is advisable.
- Monitor renal function
- Assess hydration status regularly
- Evaluate for gastrointestinal intolerance
14.2 Administration to Pregnant Women and Nursing Mothers
14.2.1 Risk-Benefit Assessment in Pregnancy
Semaglutide is generally not recommended during pregnancy. Use is reserved for situations where potential benefits justify potential risks.
14.2.2 Potential Effects on Fetal Development
Animal studies have indicated potential fetal harm. Human data remain limited, necessitating caution.
14.2.3 Excretion in Breast Milk and Recommendations
It is unknown whether semaglutide is excreted in human milk. Breastfeeding mothers should consult healthcare providers before use.

14.3 Administration to Pediatric Patients
14.3.1 Safety and Efficacy in Children and Adolescents
Clinical data in pediatric populations are evolving. Use should be guided by established clinical protocols.
14.3.2 Age Restrictions and Clinical Guidelines
Age-specific recommendations vary by indication. Adherence to regulatory guidance is essential.
15. Overdosage and Emergency Management
15.1 Symptoms of Overdose
Overdose may manifest as severe gastrointestinal distress or hypoglycemia. Symptoms include:
- Persistent nausea and vomiting
- Dizziness and weakness
- Hypoglycemic episodes
15.2 Supportive Treatment and Symptom Management
Management is primarily supportive. There is no specific antidote. Fluid replacement and symptomatic care are central to treatment.
15.3 Monitoring and Medical Intervention
Continuous monitoring of vital signs and blood glucose levels is essential. Hospitalization may be required in severe cases.
16. Storage and Stability Requirements
16.1 Recommended Storage Temperature
Sematrinity pens should be stored under refrigeration prior to first use. Exposure to extreme temperatures must be avoided.
16.2 Storage After First Use
After initial use, the pen may be stored at room temperature or refrigerated, depending on manufacturer recommendations.
16.3 Protection from Light and Freezing
Protect the medication from direct sunlight. Freezing must be strictly avoided, as it compromises structural integrity.
16.4 Shelf Life and Expiry Considerations
Adherence to expiry dates ensures potency and safety. Discard expired or improperly stored products.
17. Handling and Injection Precautions
17.1 Proper Pen Handling and Needle Disposal
Use a new sterile needle for each injection. Dispose of needles in designated sharps containers to prevent injury and contamination.
17.2 Avoiding Contamination and Infection Risk
Maintain aseptic technique during administration. Avoid sharing pens between individuals.
17.3 Rotation of Injection Sites
Rotating injection sites minimizes the risk of lipodystrophy and localized irritation.
17.4 Safe Disposal of Used Pens and Needles
Dispose of medical waste in accordance with local regulations. Improper disposal poses environmental and health risks.
18. Patient Counseling and Practical Tips
18.1 Lifestyle Modifications (Diet and Exercise)
Pharmacotherapy should be complemented by lifestyle interventions. Balanced nutrition and regular physical activity enhance therapeutic outcomes.
- Adopt a calorie-controlled diet
- Engage in consistent exercise routines
- Monitor weight and metabolic parameters

What to eat on Semaglutide
On semaglutide, focus on a high-protein, high-fiber diet with healthy fats to maximize weight loss and minimize side effects like nausea and constipation. Prioritize lean meats, fish, legumes, and non-starchy vegetables while staying hydrated with at least 80 ounces of fluid daily.
18.2 Managing Gastrointestinal Side Effects
Dietary adjustments, such as smaller meals and reduced fat intake, may alleviate gastrointestinal discomfort. Symptoms often improve over time.
18.3 Importance of Adherence and Follow-Up
Adherence to therapy is paramount. Regular follow-up ensures optimization of treatment and early detection of complications.
18.4 When to Seek Medical Attention
Immediate medical consultation is necessary if severe symptoms occur, including:
- Persistent abdominal pain
- Signs of allergic reaction
- Severe hypoglycemia
- Visual disturbances
Sematrinity Pen Injection, Semaglutide FAQ
Which brand of semaglutide is best for weight loss?
Sematrinity Pen Injection
Customers also bought





Popular Products



Similar Product
