Introduction to Unicontin-E CR
Overview of Unicontin-E CR and its therapeutic classification
Unicontin-E CR is a controlled-release formulation of theophylline, a well-known bronchodilator categorized under methylxanthines. It is primarily used in the long-term management of chronic respiratory conditions where airway obstruction is a persistent challenge.
History and clinical development of theophylline-based medications
Theophylline has a long medical history dating back to its isolation from tea leaves in the late 19th century. Over the decades, it became an essential tool in respiratory pharmacotherapy, particularly for asthma and chronic bronchitis. With advancements in formulation technology, controlled-release preparations like Unicontin-E CR were developed to maintain stable therapeutic levels and improve patient adherence.
Role of controlled-release formulations in respiratory care
Controlled-release systems provide a steady release of medication into the bloodstream, preventing peaks and troughs that often lead to side effects or breakthrough symptoms. This enhances therapeutic efficacy, reduces dosing frequency, and offers consistent symptom relief throughout the day and night.
Composition and Formulation
Active ingredient: Theophylline
The core therapeutic agent in Unicontin-E CR is theophylline, a methylxanthine derivative with established bronchodilatory effects.
Mechanism of controlled-release technology in Unicontin-E CR
The controlled-release matrix ensures gradual liberation of theophylline, maintaining optimal serum concentrations for extended durations. This minimizes fluctuations in drug levels and enhances patient comfort.
Available strengths and dosage forms
Unicontin-E CR is manufactured in varying strengths to accommodate individualized therapy. Commonly available strengths allow tailored titration based on clinical need and serum concentration monitoring.
Inactive ingredients and excipients
Besides theophylline, the formulation includes excipients that stabilize the tablet, control release kinetics, and ensure integrity of the dosage form.
How Theophylline Works
Pharmacological action as a bronchodilator
Theophylline promotes airway dilation, easing the passage of air and improving oxygen exchange. Its therapeutic role is especially vital in conditions where bronchospasm is predominant.
Mechanism: Phosphodiesterase inhibition and adenosine receptor antagonism
Its primary mechanisms involve inhibition of phosphodiesterase enzymes, leading to increased cyclic AMP, and antagonism of adenosine receptors, both of which contribute to smooth muscle relaxation and reduced airway constriction.
Effects on smooth muscle relaxation in airways
Relaxation of bronchial smooth muscle decreases airway resistance, alleviating wheezing and dyspnea. This effect is central to its clinical utility in asthma and COPD.
Secondary cardiovascular and central nervous system effects
Theophylline also exerts mild stimulatory effects on the heart and central nervous system. These properties, while beneficial in certain contexts, may contribute to adverse effects when serum levels rise excessively.
Medical Uses of Unicontin-E CR
Primary indication: Chronic management of asthma
Unicontin-E CR remains a therapeutic option for chronic asthma management, reducing airway hyperresponsiveness and preventing nocturnal symptoms.
Use in Chronic Obstructive Pulmonary Disease (COPD)
In COPD, it improves airflow and decreases exacerbation frequency, particularly in patients with persistent symptoms despite inhaled therapy.
Role in preventing nocturnal asthma symptoms
Controlled-release delivery ensures sustained bronchodilation overnight, preventing nocturnal bronchospasm and improving sleep quality.
Adjunctive therapy in patients unresponsive to inhaled corticosteroids
For individuals inadequately controlled with inhaled corticosteroids or bronchodilators, theophylline serves as an adjunct, offering an additional therapeutic mechanism.
Off-Label Uses of Theophylline
Treatment of apnea of prematurity in infants
Theophylline stimulates the respiratory center in premature infants, reducing episodes of apnea and improving oxygenation.
Use in heart failure and pulmonary hypertension (investigational)
Preliminary studies suggest it may aid in pulmonary circulation and cardiac function, though its role remains investigational.
Potential benefits in obesity hypoventilation syndrome and sleep apnea
By stimulating respiratory drive, theophylline may benefit patients with hypoventilation syndromes or sleep-related breathing disorders.
Neuroprotective properties under research
Emerging research highlights potential neuroprotective effects linked to adenosine receptor modulation, though clinical relevance requires further validation.
Dosage and Administration Guidelines
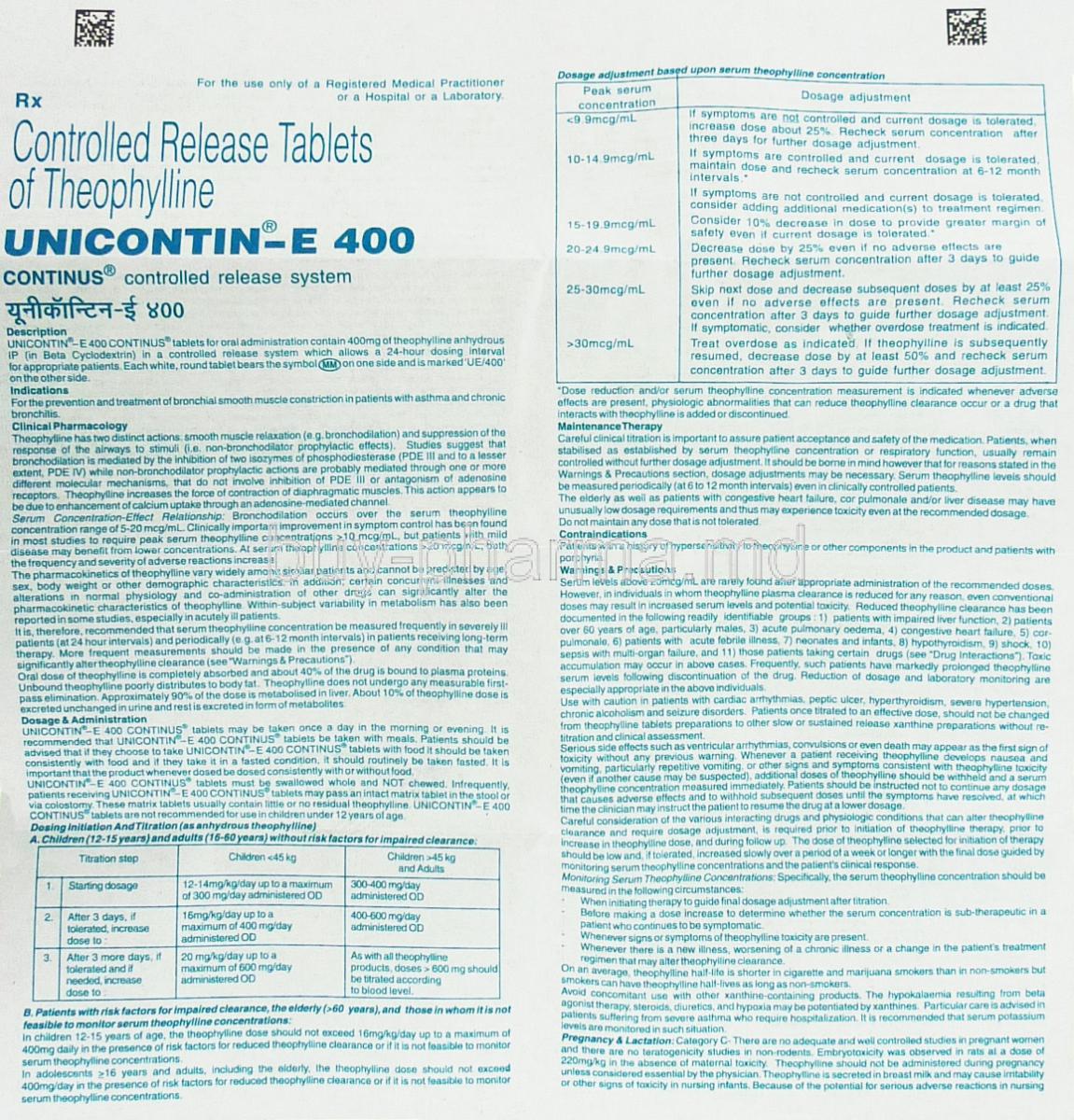
Standard adult dosing recommendations
Typical dosing involves once or twice-daily administration, adjusted based on response and serum levels.
Pediatric dosing protocols and age considerations
Dosing in children must be carefully calculated by weight, with frequent monitoring to avoid toxicity due to variable metabolism.
Individualized dosing based on serum theophylline levels
Because of the narrow therapeutic index, serum levels must be regularly measured to achieve efficacy while preventing adverse effects.
Adjustments for renal and hepatic impairment
Reduced clearance in patients with kidney or liver dysfunction necessitates dose modification and enhanced vigilance.
Administration instructions: swallowing whole tablets, not crushing
Tablets must be swallowed whole to preserve controlled-release properties. Crushing or chewing may cause rapid drug release and toxicity.
Management of missed doses
If a dose is missed, it should be taken as soon as possible unless it is close to the next scheduled dose. Doubling doses should be avoided.
Side Effects of Unicontin-E CR
Common Side Effects
- Nausea, vomiting, and gastrointestinal discomfort
- Headache and dizziness
- Insomnia and restlessness
- Mild tachycardia or palpitations
Serious Adverse Reactions
- Seizures and arrhythmias
- Severe hypotension or hypertension
- Toxicity due to narrow therapeutic index
- Allergic reactions and hypersensitivity
Warnings and Precautions
Unicontin-E CR must be prescribed with careful monitoring. The following considerations are essential:
- Regular monitoring of serum theophylline levels to avoid toxicity
- Risk of drug accumulation in hepatic or renal impairment
- Caution in individuals with seizure disorders or cardiovascular abnormalities
- Awareness of lifestyle factors such as smoking and caffeine consumption, which alter drug metabolism
Contraindications
- Known hypersensitivity to theophylline or related xanthines
- Acute myocardial infarction and severe arrhythmias
- Active peptic ulcer disease
- Severe uncontrolled seizure disorders
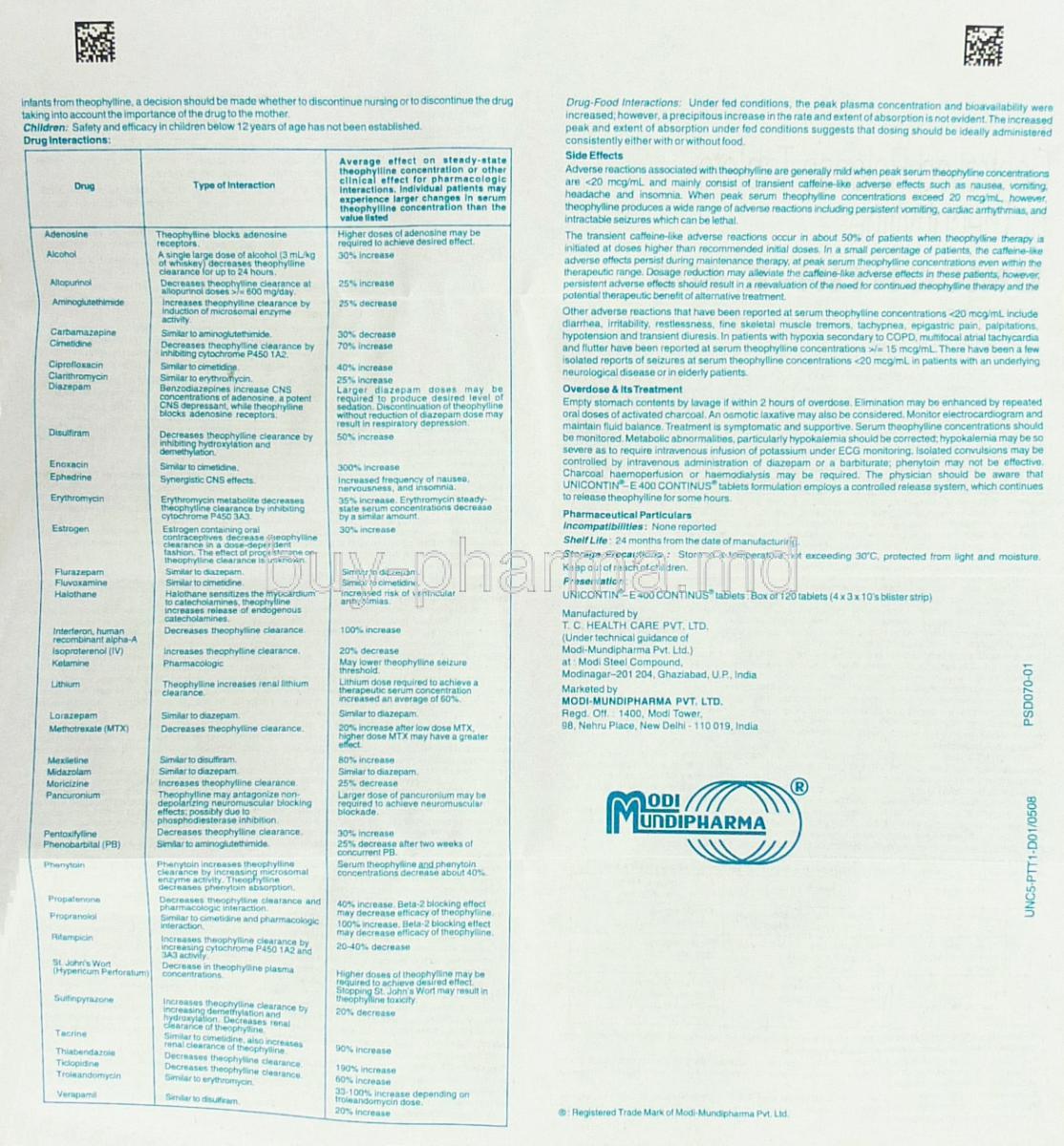
Drug Interactions with Unicontin-E CR
Interaction with antibiotics (e.g., macrolides, quinolones)
Theophylline clearance can be significantly reduced when taken alongside antibiotics such as macrolides or quinolones. This reduction elevates plasma concentrations, increasing the likelihood of adverse reactions such as nausea, arrhythmias, and central nervous system disturbances. Clinicians often recommend careful monitoring of serum levels when these combinations are unavoidable.
Increased risk with CYP1A2 and CYP3A4 inhibitors and inducers
Theophylline metabolism primarily occurs through cytochrome P450 enzymes, particularly CYP1A2 and CYP3A4. Interactions include:
- Inhibitors (e.g., fluoroquinolones, ketoconazole, erythromycin) that raise drug levels and enhance toxicity risk.
- Inducers (e.g., rifampicin, carbamazepine, phenytoin) that accelerate metabolism, diminishing therapeutic efficacy.
Interaction with antiepileptics, cimetidine, and fluvoxamine
Co-administration with antiepileptic drugs may alter clearance rates, complicating seizure management. Cimetidine and fluvoxamine are potent inhibitors of theophylline metabolism and require dosage reduction to avoid harmful accumulation.
Reduced effectiveness with smoking or high caffeine intake
Smoking induces hepatic enzymes, resulting in faster clearance and reduced therapeutic effect. Excessive caffeine intake may potentiate the stimulant effects of theophylline, heightening risks of insomnia, tremors, and palpitations.
Administration in Special Populations
Elderly Patients
Age-related physiological changes can profoundly influence theophylline pharmacokinetics. Elderly individuals exhibit reduced clearance, rendering them more sensitive to toxic effects. Dose titration should proceed cautiously, with frequent therapeutic monitoring.
- Enhanced sensitivity to arrhythmias
- Greater risk of gastrointestinal intolerance
- Requirement for slower dosage escalation
Pregnant Women and Nursing Mothers
Theophylline crosses the placental barrier, potentially affecting the developing fetus. High levels are associated with intrauterine growth restriction and neonatal irritability. Furthermore, the drug is excreted into breast milk, necessitating vigilance when prescribed during lactation.
- Fetal exposure may result in tachycardia or jitteriness
- Breastfed infants can develop mild toxicity if maternal levels are uncontrolled
- Close supervision and serum level assessment are recommended
Children and Infants
Theophylline remains a therapeutic option in pediatric asthma, though its use requires precision due to wide inter-individual variability in metabolism. In neonates, it is occasionally used to manage apnea of prematurity, stimulating respiratory drive.
- High variability in clearance rates increases risk of overdose
- Small dosing errors may lead to severe toxicity
- Requires regular serum concentration monitoring
Overdose and Toxicity Management
Signs and symptoms of acute theophylline overdose
Toxicity presents with a constellation of alarming symptoms, including persistent vomiting, tachyarrhythmias, seizures, and profound metabolic disturbances. These events demand immediate medical intervention.
Seizures, arrhythmias, and metabolic disturbances
Convulsions and life-threatening cardiac arrhythmias represent the most severe consequences of overdose. Electrolyte imbalances and metabolic acidosis further complicate the clinical picture.
Emergency interventions: gastric lavage, activated charcoal, anticonvulsants
Emergency management typically involves rapid decontamination through gastric lavage or repeated doses of activated charcoal. Benzodiazepines or barbiturates may be administered to control seizures, while supportive cardiac care is essential.
Importance of serum theophylline concentration monitoring
Serial blood level measurements remain the cornerstone of overdose management. They guide therapeutic decisions and confirm the resolution of toxic accumulation.
Handling and Storage Precautions
Proper storage conditions: temperature, light, and moisture protection
Unicontin-E CR tablets should be stored at controlled room temperature, away from direct light and humidity, to preserve their controlled-release properties.
Safe handling to prevent accidental pediatric ingestion
The medication must be kept out of children’s reach, as even small ingestions can lead to critical toxicity in young patients.
Shelf life and stability information
The product retains its potency within the manufacturer’s recommended shelf life when stored under appropriate conditions. Tablets should not be used beyond their expiration date.
Disposal of expired or unused medication
Expired or unused medication should be discarded following pharmacy or local authority guidelines. Flushing into water systems is discouraged to avoid environmental contamination.
Important Precautions in Long-Term Therapy
Need for periodic liver and kidney function tests
Long-term use necessitates periodic evaluation of hepatic and renal function to ensure safe metabolism and excretion of the drug.
Monitoring for changes in smoking habits, diet, or medication regimen
Alterations in smoking status, dietary habits, or concomitant medications can drastically modify theophylline levels. Regular reassessment of dosage is crucial.
Education on adherence and recognizing early toxicity symptoms
Patients should be instructed to adhere strictly to prescribed dosing schedules. They must be vigilant for early signs of toxicity, such as persistent nausea, restlessness, or palpitations.
Importance of avoiding sudden discontinuation without medical guidance
Uncontrolled cessation may precipitate exacerbations of asthma or COPD. Gradual adjustment under medical supervision is strongly recommended.
Unicontin
This is for respiratory issues.
Unicontin-E
I am pleased with this product. Shipment arrived in a timely manner.
I will be a loyal customer!!!
Awesome customer service and fast shipping. I am very pleased with this product and will try others as well.I especially liked the email showing me the other sites.
Unicontin-E CR, Theophylline FAQ
Customers also bought




Similar Product